
This is a story with two subjects. On the one hand, we have another blatantly irresponsible organization failing to take the most basic safety precautions; on the other, we have the deadly results of ignorance. It’s far from the only tale of its kind; the list of radiological accidents in developing or less-developed countries is depressingly long.
In order to explain how Goiânia happened, we need to touch briefly on the nature of the machine that started the disaster. Radiotherapy for cancer can take many forms: teletherapy (now known as external beam radiotherapy), where the source of radiation is outside but focused on the body; brachytherapy, where sealed radioactive sources are placed inside or next to the part of the body needing treatment; and systemic or unsealed source radiotherapy, where a soluble radionuclide is injected or ingested into the body. Mostly when people think of radiotherapy they think of external-beam/teletherapy machines with the rotating gantry and patient couch.
These days EBRT is mostly performed using linear accelerators, which produce a powerful beam of beta radiation (electrons) or X-rays with the push of a button and do not require dangerous radioactive source capsules, but in the early days of teletherapy they didn’t have that option. The two most common radioactive substances used as teletherapy sources are cobalt-60 and cesium-137. Both of these will kill you quite quickly if you pick them up in your hands: the machines using them rely on massive lead shields to limit the radiation to a controlled, collimated beam. The cesium-137 source in the Goiânia accident was filled with highly soluble, highly dispersible powder, rather than pellets of metallic solid material. This would prove to be important.
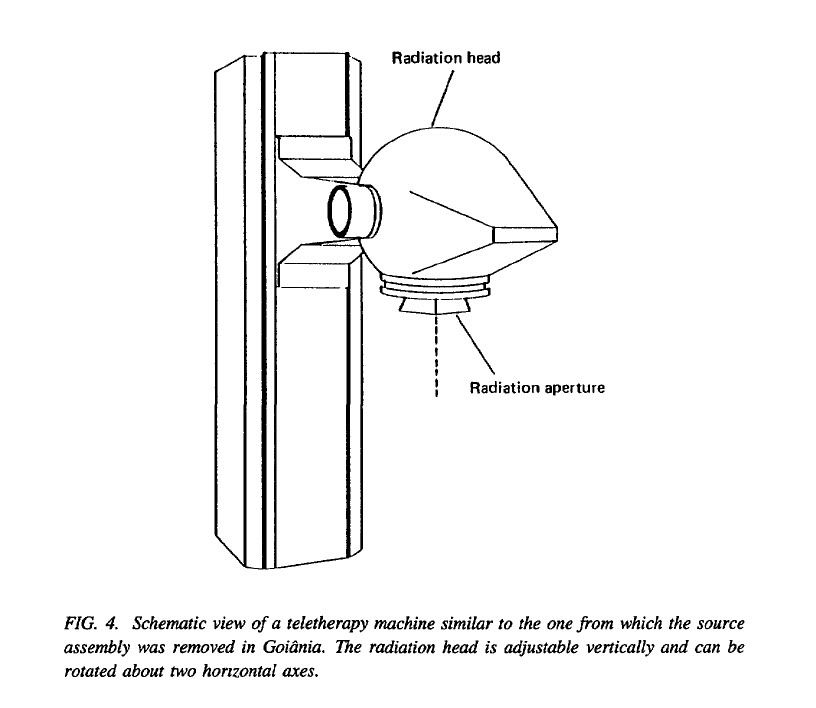
The unit involved in the accident was a Cesapan F-3000, a 1950s Italian design containing what was probably a source capsule manufactured in America in the seventies. It would have looked a little something like this (images from IAEA report). The rather ominous-looking head was capable of moving up and down on its support pillar and rotating through a couple of horizontal axes, and contained the source capsule in a rotating assembly that could move to line up the window in the capsule with the radiation aperture in the head, as illustrated here. The window in the shielding of the capsule, through which radiation could escape, was made of iridium. According to the International Atomic Energy Agency (IAEA) report, the source itself was of standard international dimensions and potency.
This machine was left in the derelict premises of a private radiotherapy clinic in Goiânia, capital of Goiâs State, Brazil, after the partnership that owned it dissolved toward the end of 1985; a cobalt teletherapy unit from the same clinic premises was removed and transferred to a new facility, but the cesium unit stayed where it was. We aren't sure why.
Vagrants used the gutted building to shelter in; wildlife came and went, and the Cesapan F-3000 stood there growing quietly more obsolete. It is perhaps surprising that it remained unmolested for two years before enterprising locals considered its potential scrap value.
On September 10, 1987, two men, A and B, began to try to dismantle the machine. It took a while and several attempts, but by September 13 they'd managed to extract the rotating assembly from the massive shielding of the radiation head. Outside this shielding, the unprotected source was giving off 465 rads an hour, or 4.65 Gray if you want to be modern about it. For comparison, the accepted annual radiation dose for non-nuclear-workers in the USA is between 1 and 5 millisieverts, or ~ 0.001 to 0.005 Gray.
They put the assembly in a wheelbarrow and took it to A's house; A had suggested salvaging the machine for scrap in the first place. That day, both of them began to vomit; over the next few days, B developed diarrhea and edema of his hand, which subsequently would develop into a burn corresponding to the size and shape of the window in the source capsule. They attributed their symptoms to something they'd eaten, and in fact when B saw a doctor he was told his symptoms were due to a food allergy and he was to take it easy for a week.
The real horror begins
In the days between September 13 and September 18, A had been tinkering with the rotating source assembly, which he'd dumped under a mango tree in his yard. He was trying to get the source capsule free of the assembly. At some point he managed to break the iridium window of the source with a screwdriver.
He thought that perhaps the intensely radioactive cesium thus exposed might be gunpowder, and tried to light it.
On the 18th he managed to get the breached source free of the rotating assembly, and sold the whole mess to a third man, C, who owned a junkyard nearby. That night, C went into the garage where the bits were stored and noticed that the stuff in the broken capsule was emitting a blue glow, and brought the capsule into his house to show it to his wife. Because it was so pretty and so strange, they thought it might be valuable, or have supernatural powers, and invited their friends over to have a look. On the 21st one of these friends dug out some of the powder with a screwdriver and took it away with him to give to his family and friends. Quite a few of them rubbed it on their skin like body glitter. C received a total dose of 7Gy and survived. His wife (5.7 Gy) would not.
I know this reads like a horror novel. It gets worse.
More people were (unsurprisingly) suffering the symptoms of acute radiation sickness: C's vomiting wife was examined at a local hospital, diagnosed with food poisoning, and sent home to rest. Her mother came over to take care of her, and took home a dose of 4.3 Gy.
Two of C's employees were tasked with removing lead from the remnants of the assembly, and worked on it from September 22 to 24. Directly exposed to the breached source capsule, they would be among the four victims who did not survive.
The last of the four fatalities was C's six-year-old niece, whose father had visited C and taken away some of the glowing powder. This was left on the table and handled by the family during meals. The little girl had played with the powder and put her fingers into her mouth. According to one source, when international medical teams arrived to treat the victims, they found her in an isolated room in the hospital because the staff were afraid to go near her.
On the 23rd, B was admitted to hospital: his skin lesions were diagnosed as related to some exotic disease, and on the 27th he was transferred to the Tropical Diseases Hospital.
The authorities finally become aware of the accident
After doing its damage to C's friends and family, the source and rotating assembly were sold to a second junkyard. The sudden epidemic of vomiting and diarrhea among their acquaintances was not lost on C's wife, who became convinced that the glowing powder from the capsule was responsible for all the sickness. On the 28th, ten days after the source was transferred to C's ownership, she and one of C's employees went to collect the remains of the source and rotating assembly from the second junkyard, put it in a plastic bag, and took it by bus to a hospital, spreading contamination as they went. The employee and C's wife presented a doctor, P, with the source in its bag, and she told him that it was "killing her family."
By now the employee who had carried the bag was developing a serious radiation burn on his shoulder, where it had rested, and he and C's wife were sent to the Tropical Diseases Hospital, where B and several other contamination victims had been sent for treatment. One of the doctors at the TDH was beginning to suspect that in fact the nearly identical symptoms of this whole cohort of patients could have been caused by radiation, and he contacted a colleague who had independently been contacted by Dr. P. Dr. P had initially thought that the bag contained bits from X-ray apparatus, and became wary of it, moving it outside the facility (and thus probably saving his own life).
The doctors at the TDH had another look at the patients, with the mysterious bag's contents in mind, and agreed that it would be a good idea to contact the state department of the environment; when they did, it was recommended that a medical physicist examine the package.
On the 29th they found a medical physicist, W. He found a radiation monitor used for uranium prospecting, which had a range of 0.03–30 microgray/hour, and set off for the hospital where the source was currently located: quite some distance away he noticed that the monitor was pegged no matter where he pointed it. He assumed it was malfunctioning and went back to fetch a different one, which showed exactly the same thing as soon as he turned it on.
At this point W realized that something was desperately wrong. At the hospital, Dr. P had become sufficiently concerned about the source in its bag that he had called the fire department, which had arrived and was preparing to chuck the whole thing into a handy river; W arrived on the scene just in time to prevent this. He convinced them to evacuate the hospital and make sure no one else got near it, and after talking with Dr. P they set off together to C's junkyard–where the monitor again read off the scale.
The official response begins
W, among others, managed after some effort to notify the secretary of health. Once the authorities had been convinced that yes, in fact, this was a huge deal and would require evacuation of a large number of people, steps began to be taken with considerably greater speed. The physicist and physician at the radiotherapy clinic's new location were notified, and the source was tentatively traced to the abandoned clinic and the cesium unit.
Civil defense forces were notified; the TDH was informed that a number of patients were contaminated; the known sites of contamination were resurveyed with equipment from the radiotherapy clinic; an emergency receiving and decontamination facility was set up in a local stadium. W, the physicist who had initially discovered the contamination, was contacted by an individual who had intended to cut up the source for C with an oxyacetylene torch (but had luckily forgot), who explained several useful details to the investigation.
International teams were sent in to decontaminate and treat the victims of the disaster. There is not a great deal that can be done in cases of radiation sickness: therapy consisted of dealing with the acute period of bone marrow suppression and subsequent immune deficiency, treating the burns, removing radiation from the body (decorporation), and general support. It's rather terrible to consider that many of these patients recontaminated their skin repeatedly by sweating; the cesium in their bodies found its way out in everything. Chelation with Prussian blue helped a significant number of the victims, a point which recalls the hopeless suggestion of treating Louis Slotin with methylene blue after his deadly exposure to plutonium criticality.
The final count of persons with significant contamination, out of the hundred thousand screened, was two hundred and forty-four. Most of those were lucky and received fractionated doses--spread over a long time period, giving the body's tissues a chance to attempt to recover from the damage. Some were not. The dead of Goiânia had to be buried in lead coffins surrounded by concrete.
Cesium didn't just destroy people in Goiânia, it destroyed property and livelihoods. Seven houses had to be demolished, so badly contaminated they could not be made safe. Topsoil was removed by the ton. In total 85 houses had to be decontaminated.
More than anything Goiânia stands as a blazingly vivid example of the importance of keeping sources secured. A number of factors conspired to make this accident as deadly as it was: criminal negligence on the part of the radiotherapy clinic which failed to remove and secure the capsule from the teletherapy unit, the nature of the radioactive material--its mysterious and magical blue glow entranced people, significantly increasing the scope of the disaster, and its powdery nature was easily dispersed and easily soluble--and the remote location of the disaster site. But the lesson of Goiânia applies to all source capsules, not just cesium in remote and unsophisticated locations.
Sadly, it's not a lesson that's been learned particularly well. In the years since Goiânia, unsecured radiation sources have caused at least four radiological accidents around the world. In Samut Prakarn, Thailand, a disused cobalt-60 teletherapy head was partially dismantled, taken from an unsecured storage location, and sold as scrap metal–in February of 2000. It's still happening. It will continue to happen as long as those in charge of radiation sources fail in their responsibility to keep them secure.
In many ways the eighties were a great time for death by radiation. You had Chernobyl, you had the 1983 Ciudad Juarez accident in Mexico–eerily similar to Goiânia–you had the Therac-25 linear accelerator deaths; but it hasn't stopped. People need to pay more attention to things that have happened, if they want to live very much longer; and people who take the responsibility to treat their fellow humans with lethal radiation must take the responsibility to prevent their fellow humans from dying of it.
Information in this article is from the IAEA report on the incident, available at www-pub.iaea.org/MTCD/publications/PDF/Pub815_web.pdf, and from Wiki.
Friday, June 26, 2009
{kind=link}
{kind=link}
Tuesday, June 16, 2009
“No, I cannot say that I have:” a clueless crew and a firetrap ship, the SS Noronic
Nothing can beat the Apollo 1 launchpad fire in terms of flame propagation speed, but the cataclysmic fire that destroyed the SS Noronic in 1949 as she sat beside the docks of Toronto’s Pier 9 was impressively rapid nonetheless. The focus of investigations into the Noronic fire was not the point of origin--that was fairly obvious from eyewitness accounts--or the actual source of ignition: it was the rather horrifyingly laissez-faire attitude of the crew members regarding what to do in the case of a fire in dock.
The official "Report of Court of Investigation into the Circumstances Attending the Loss of the S.S. Noronic" contains quite a lot of direct quotes from examination of the various officers, included into the narrative to make the point abundantly clear: there was no official instruction given to crew members regarding their duties in case of fire in dock, and no attempts made to develop or distribute same, because “the ship had been running from 1913 without mishap.”
The Noronic, built (as mentioned) in 1913, was a cruise and package freight ship plying the Great Lakes. She had two sister ships, the Huronic and the Hamonic; this last, suffering under an even sillier name than Noronic, burned out in 1945. No apparent lessons were learned from the loss of the Hamonic, as demonstrated very clearly in the behaviour of the Noronic’s crew prior to and during the disaster.
She was vast for the time, capable of carrying six hundred passengers and two hundred crew on her five decks, and considered one of the most beautiful and luxurious cruise liners in Canada. Part of her luxury came from the fact that her interior walls were paneled in beautifully polished wood, into which thirty years of lovingly applied lemon-oil varnish had soaked. Some of the wood (the passenger accommodations on D deck) was painted rather than varnished, but the majority of the walls in the upper decks and communal areas were treated with this highly flammable oil.
She was also, being built prior to regulations passed in 1939, lacking the requisite fire-resistant bulkheads the regulations called for. The Chairman of the Board of Steamship Inspection was allowed to exempt existing ships from compliance with the regulations where it was “impracticable or unreasonable” to retrofit the ship to comply. In this case it was rather obviously “expensive” to do so, and Noronic remained a totally period-accurate vessel.
The series of legal loopholes through which the Noronic sailed to escape the installation of vital safety systems is impressive. Not only was she allowed to go around without fire-resistant bulkheads, she also did not have to comply with Regulation 3 of section 405 (1) c of the Canada Shipping Act, requiring “every ship…which is engaged on an international voyage, [to be provided with] an approved fire alarm or fire-detecting system which will automatically register at one or more points or stations in the ship, where it can be most quickly observed by officers and crew, the presence or indication of fire in any part of the ship…not accessible to a fire patrol system.”
Fire patrol meant that the crew was detailed to regularly make exhaustive rounds of the ship throughout the day and night to catch any hint of fire on board; the regulations stated that “all spaces in a passenger ship, except such spaces as cargo spaces, baggage and store rooms, may as a general rule be regarded as accessible to the patrol,” thereby exempting them from the requirement that an automatic alarm or detection system be fitted. Noronic was not considered international, as she only puttered around on the Great Lakes—an “inland voyage.” Even had she been considered “international” due to her route between Canada and the States and thus required to comply with Regulation 3, the Board of Steamship Inspection ruled in 1938 that Regulation 3 only applied to ships making international voyages on the ocean. Either it didn’t apply, or it didn’t apply.
Noronic did in fact have a manual fire alarm system that ran off batteries, of the in-case-of-fire-break-glass type. This alarm rang bells located a) in the officers’ quarters, b) on the port side of D deck, and c) in the engine room on E deck, registering the location of the pulled alarm. It did not activate the klaxons located around the ship which would alert passengers and crew to an emergency: in order to sound those someone would have to go up to the pilot house above A deck to manually flip the klaxon switch. The first and second officers informed investigators that it was “the duty of the officer on watch, upon hearing the bell alarm, to proceed to the locality from which the alarm had been given for the purpose of investigating whether the fire was serious enough to require the sounding of the klaxon alarm and, if he so concluded, then to return to the pilot hours above A deck where he would throw the switch which sounded the klaxon horns. If the officer on duty was away from the pilot house, the wheelsman who should be there was expected to find the officer on duty and report to him as to the locality at which the alarm had been sounded. To obtain this information he would first have to go to the bath-room in the mates’ quarters where the indicator was located.”
I quote the report again directly: It is, of course, obvious from the above that considerable time might be lost between the giving of the alarm at the point where the fire was first discovered and the giving of the klaxon alarm which could only be sounded from the pilot house.
No shit.
It goes on like that. There were supposed to be hydrants located all around the ship so that “at least two powerful jets of water can be rapidly and simultaneously brought to bear upon any part of each deck or space occupied by passengers or crew,” but the inspectors thought, eh, it’d be good enough if you could just run a hose down from the deck above if there weren’t enough hydrants on any given deck (even though the actual wording of the regulations states that “the hydrant shall be so placed on each deck that the fire hoses may be easily coupled to them").
It's apparent that nobody in a position to enforce safety regulations ever actually thought a fire could break out on the Noronic. Certainly they made every effort to weasel out of providing even the most basic of safety systems, taking advantage of the fact that as Noronic was merely sailing on a lake and not the ocean she did not strictly fall under the regulations requiring fire patrol. Whether this is due to some unknown dangerous quality in salt water as opposed to fresh is not explained. The report mentions tartly that in the judge’s opinion the regulations requiring ships to be equipped with working hydrants and extinguishers imply that there also should be crew members provided by the ship’s owner to use the aforementioned apparatus. Without an automatic fire detection system or a sprinkler system on board, Noronic really could’ve used a fire patrol. What they got was this:
Two crew members designated “Special Officers” switched off at 6-hour intervals to walk around the ship with a time clock and punch a series of keys located at various points on board “on the hour.”
Yeah. In 1942 Canada Steamship Lines issued a list of duties to be completed by the Special Officers, including:
“Each night from 9:00 PM until 6:00 AM the watchman clock shall be punched punctually on the hour. The dials are carefully checked by the Purser and the reason for not punching or the dials not being marked must be explained satisfactorily by the officer. During the round of punching, it is your duty to stop any excessive noise by passengers that are boisterous…Upon completion of your round and all passengers are quiet [sic], return to the rotunda where you are easily found should you be needed…”
The round of time-clock punching took about 15 minutes, which meant that for 45 minutes out of every hour there was pretty much zero fire patrol going on. One of Noronic’s Special Officers said that he thought he wasn’t supposed to do the patrol at all when the ship was in port, but remain instead at the gangplank; the other one understood his duty to be completing the rounds each hour and then returning to the gangplank. In fact neither of them were on board the night of the fire: both Special Officers’ rounds were conducted by a pair of wheelsmen who took the shortest possible routes between the time clocks.
This lack of clarity amongst officers and crew comes up over and over again throughout the investigation. This officer understood that this other officer was supposed to do something, but didn't check with anyone to see if this was in fact the case; that officer thought he was supposed to do this other thing but in point of fact was supposed to be somewhere else entirely and had no idea what to do in case of emergency. The card in the passengers' accommodations regarding fire stated confidently that the ship was equipped with "modern fire prevention apparatus" and patrolled "day and night by experienced watchmen." Or inexperienced wheelsmen doing the watchmen's jobs for them, either way.
Fire and lifeboat drills were regularly held on board the Noronic when she was moored in Duluth. Every Tuesday at ten in the morning, the signal was given for fire drill and the crew members assigned to "fire stations" (hydrants) gathered at their posts. The objective of the drill was to get to the hydrant, get the hose down from its rack, and couple the hose to the hydrant. Sometimes on the outside fire stations they'd squirt the hoses overboard, but obviously not indoors. A few crew members were expected to get the extinguishers down and wave them about, maybe discharge one or two. That was it for fire training of the crew.
In 1945, the General Manager at Canada Steamship Lines was apparently made aware of the fact that his ships were practicing a thoroughly useless excuse for a fire drill, and sent out a memo with an updated list of rules. The memo stated that the enclosed Lifeboat and Fire Drill Regulations were (I quote) serious business, and that masters of all passenger steamers must study them carefully and instruct all crew members accordingly. Let's see how the Norons did:
1) MUSTER STATIONS: The Master will designate locations of muster stations throughout the ship to which members of the crew will report for lifeboat and fire drills (and make sure all crew members know where these stations are and which signals call for them to muster).
1) a ALARM SIGNALS: General or Fire Alarm is indicated by one long, three short, one long blasts on whistle or alarm. Proceed at once to fire drill assigned station. Man Boats Alarm is indicated by General Alarm followed by two short blasts on whistle or alarm. Proceed at once to boat drill assigned station.
The Noronic's crew members each carried a blue card on which was printed his crew number, his fire station number, and his boat number. It clearly states the types of alarm and what one should do upon hearing them. However, in practice, the fire drill signal was a continuous blast on the klaxon horns, while the lifeboat drill signal was identical to the official "general or fire alarm" signal. Crew members had to learn to ignore the info on the blue card.
Passengers did not take part in either drill. The only information they received on what to do in case of fire was on the instruction cards in their rooms. The crew were the only ones who had any idea of emergency procedures, and their grasp on same was tenuous at best.
2) MUSTER LISTS: The Master will have a muster list prepared including the information of all crew members and their muster stations, as well as "full particulars" of the signals required to call members of the crew to muster. This list shall be posted in conspicuous places throughout the ship including the crew's quarters and every officer's room.
There was no such thing as a "muster list" on board the Noronic, nothing signed by the Master, and nothing hung in any officer's room. A "chart" of crew members apparently hung in the maids' quarters, in the crew's stairway aft, on either B or C decks, and in the crew's rec room. The first officer, Gerald Wood, used this chart to prepare a list of crew members and their blue card numbers, boat numbers, and hydrant numbers, and gave a copy to the chief steward. The captain was completely ignorant of all of this and only knew about the typed list because he looked over Wood's shoulder as he was filling it out. Who's on board? Whose job is it to do what? Who knows?
3) MUSTER CARDS: A card indicating the muster station for each crew member must be placed in his berth in such position that it cannot be obscured by baggage or clothing.
The only thing remotely similar to this in use on the Noronic was the blue card, which was kept wherever the crew felt like keeping it.
There was also a rule stating that the Master had to appoint Senior Officers to various parts of the ship in order to help direct passengers to their muster stations if necessary. Here is where the testimony really gets interesting: Captain Taylor said that he'd allocated the first officer to C deck, second officer to A deck, third officer to B deck, and chief steward and purser to D deck. Wood, the first officer, denies any allocation was made, and then proceeds to flip-flop like a gaffed pike (unsurprisingly, he stated that he had never seen or heard of the Serious Business memo):
Q: Was there any allocation that you know of of senior officers allocated to certain locations for the purpose of mustering passengers?
A: No there was not.
Q: Did you make any allocation?
A: No.
Q: Did anyone else to your knowledge?
A: Not that I know of.
Q (really trying here): Now I want to be fair with you. I thought the Captain did say to us that he had allocated certain senior officers in accordance with this and he said the allocation was the chief officer to C deck....do you know anything about that?
A: Well yes, I would be in charge of C deck.
Q: (wondering what he's smoking): Well that is what he told us, that you were in charge of C deck--then must that not mean that you were allocated in some way to C deck?
A: Yes, I would be allocated.
Q: How would you be allocated and what instructions did you have with regard to C deck?
A: I think by this chart [which indicated his duty was free to move about the ship].
(some back and forth about whether or not this allocation is the same as on other ships)
Q: Now what do you say as to whether or not any station was allocated to you as the first officer under this regulation?
A: Well he may have told me to go to my allocation on C deck.
Q: (between clenched teeth) Well he may and then I suppose he may not, but I am trying to get from you whether he did.
A: Well I have been there a number of years.
Q: Then is your statement to me that you do not know whether the Captain in the case of fire had told you that you were to go to C deck?
A: I am pretty sure--I might say that the captain did not tell me this year. He could have back in 1944 or 1945.
Q: Did you always go to C deck on fire drill?
A: No, I go all over the ship.
Q: Then you were really not allocated to C deck?
A: Not to stay there.
Q: Well was anybody allocated to C deck?
A: Well I think the officers were free--wherever we could be the most help.
This confusion is heightened by "the chart," which states that Wood was in fact in charge of deck A. Balancing out various testimonies against one another it becomes abundantly clear that this "chart" had become so obsolete by 1949 that it had nothing to do with any organization or lack thereof on board the ship and in fact the captain had no idea it existed at all. We are dealing with governmental levels of confusion here. The captain and first officer, when asked about duties to be performed by the officers and men at the fire hydrant stations, contradicted one another and made up answers to explain what the rest of the crew not assigned to hydrants would be doing (running away, is my guess).
The slipperiness of officials when faced with questions about the Noronic extends way up the ladder. General Manager of the line Captain Reoch had to admit under examination that in fact when he wrote the Serious Business memo he did not take into consideration the fact that, if a fire occurred while the ship was tied up to a dock, directing all the passengers to the muster stations on C deck would not do them a blind bit of good as the only gangplanks to the dock were on E deck three floors below. "Was it your intention under these rules when you drew them up, that in the event of a fire at a dock, the passengers from D deck would go up or be directed to C deck and then go back down to D [and then E] deck to get off onto the dock?" he was asked. After some squirming and repeated requests to answer the question, Reoch finally admitted that he didn't think that the rules he'd indicated would be followed in case of a dockside fire--or, more accurately, he'd not bothered to consider the possibility.
The really damning bit is when they are asked why they didn't increase the number of crewmen on fire patrol while the ship was tied up. "If there had of [sic] been any signs of an emergency, yes, but there was no reason why they would have. I can't see any reason why they would."
Maybe because you're in a floating firetrap lacking rudimentary safety systems, steeped in decades' worth of flammable varnish, and inhabited by people who are coming back from Toronto bars drunk off their tits and probably waving around lit cigars?
There was no way of knowing which crew members were on or off the ship while she was in port, as they were free to go ashore at any time they were not on duty. If there had been any organization amongst the crew for dealing with emergencies, it went directly out of the porthole as soon as crew members began to go ashore unremarked.
So we have the perfect setup for disaster. On the night of September 17, 1949, something in a linen closet on C deck aft caught fire. The closet contained bed linen, towels, and cleaning materials, as well as a box for rubbish and wastepaper collected from the cabins, and a switchbox controlling some of the stateroom lights. The presence of the box is controversial: a maid stated that the rubbish box was never placed in the linen closet; the chief steward said it might have been there, and an eyewitness stated that it was there. If the fire was due to a smouldering cigarette butt, this box would have represented a perfect point of origin. Passengers mentioned seeing maids smoking cigarettes in the linen closet during the voyage; in the absence of a major electrical fault it seems likely although not certain that a carelessly discarded butt was responsible for killing somewhere between 118 and 139 people.
A passenger, Don Church, noticed a haze in the starboard corridor around 2:30 a.m. and followed it to the linen closet, where he saw smoke coming from the sides and top of the locked closet door. He heard a faint crackling, rustling noise, and assumed someone was inside; this would have been the fire talking to itself. Church, unable to open the door, ran forward yelling that the boat was on fire and encountered the head bellboy, Earnest O'Neill. O'Neill ran back with him to the locker, whereupon their stories diverge: O'Neill stated that he ran back to the steward's officers to fetch the closet key, then went to fetch a fire extinguisher before unlocking the door. Church stated that he just unlocked the door as they arrived.
They opened the door and saw that the wall was in flames and a hanging sheet was beginning to burn. The extinguisher barely slowed it down: almost as soon as the door was opened, flames poured out along the ceiling, feeding on the beautifully polished wooden paneling. Church and O'Neill went for a fire hose, but when Church opened the valve nothing came out. At this point he thought sod this for a game of soldiers and went off to fetch his family and got the hell out of it.
O'Neill only now broke the glass on the fire alarm and ran down to E deck to find a wheelsman and inform him of the fire. It's uncertain how much time really elapsed between the discovery of the fire and the sounding of the alarm, but time was definitely lost in trying to put out the fire with ineffective means. If O'Neill had sounded the alarm at once instead of messing about with extinguishers, several senior officers could have responded at once and taken charge of the fire equipment: C deck was the most well-staffed in terms of hydrant stations. He didn't. The fire raged out of control.
The wheelman O'Neill had woken in turn woke Wood, who quickly sounded the klaxon alarm and pulled the whistle, which stuck open and drowned out the klaxons. By now the starboard side of the boat was "full of fire," and he could not go aft farther than the first three cabins on the port side, where he "banged on the windows" and shouted.
Just before Wood sounded the whistle, a night watchman on the pier was appalled to see flames breaking through a window on the ship's starboard side. He ran inside and called the fire department and gave the alarm, then called the police; someone else standing at the door told him to call for ambulances as well. After he'd told the police to send all the doctors and ambulances they could, the watchman--a Mr. Harper--went back outside to find a mass of flame engulfing the starboard side of the ship. Now the whistle was blowing--Wood had sounded the alarm--and the fire department was arriving. By now it was 2:41 a.m., eleven minutes since Church first saw the smoke, and half the ship's decks were on fire.
The man who had told Harper to call for ambulances was one of the first to escape the burning ship. He had seen people badly burned--a woman with her hair burned away, people with faces and arms scorched and bubbling. It was still only minutes after the fire had begun, and already it was lethal.
The captain was informed of the fire some time between 2:30 and 2:35, according to his testimony, but the times don't match up; he claims to have gone out to yell for help from the outside deck and observed people on the pier, but Harper the watchman had seen the fire begin to erupt and made the alarm call when there had been no other people on the dock.
There is considerable flip-flopping from Wood regarding the instructions he had given to the crew members as to what they ought to do in case of fire: should they notify the officer on watch or just any officer, should they use a hose or an extinguisher first, did he actually tell them anything at all. "Would this be fair," he was asked, "and now correct me if I do not say it correctly--that so far as the education of the crew in the event of fire was concerned, all they had was what they saw on the printed chart in the crew's quarters, which took them to their various stations in the event of hearing the alarm--is that all they had--apart from what you have just said as to what you might have told any particular member of the crew--does that cover the whole field?"
"Yes, that covers it."
There was no organization, and therefore there was no clear and evident list of duties for each member of the crew to perform. Some of the fifteen men on duty tried harder than others to waken passengers and shepherd them over the side on ropes and Jacob's-ladders; by now the fire department was there en masse and trying to reach the ship with aerial ladders, but so many people leapt on the first of these--Aerial No. 5--that it snapped and spilled the lot of them into the harbour. Other passengers leapt straight into the water, some of them screaming as they burned, some of them in eerie silence. Many people were asleep when the fire broke out, and woke only to find their cabins ablaze and the only way out blocked by a window-screen they could not break; some were pulled from burning cabins from the outside by crew members or fellow passengers who had broken the screens away.
GenDisasters offers a collection of quotes from eyewitnesses. Mildred Briggs of Detroit, one of the survivors, said the flames spread as if in a matchbox. "The fire just welled up along the corridors and spread faster than any fire I've ever seen," she said.
"There was a mob of men and women surging back and forth," said another survivor, Alberta Agia of Detroit. "Men were pushing women around, and many were knocked to the floor. The screaming filled the air. There was so much panic that I don't know how these people found anyway to safety. I slid down a rope."
Men rushed out in their nightclothes. One man got ashore naked.
Henry Maurer and his wife were sound asleep when someone pounded the door. When they reached the outside rail, his wife started down a rope ladder, "but it became horribly twisted from so many trying to get on it. She got tangled and trapped. I swung down on a rope to her side and got her free, and we both managed to get to the dock."
Sylvia Carpenter of Detroit said she screamed and headed for the outside rail when she saw smoke and flame billowing along the passageways.
"A rope was tossed over the rail and I put a hitch knot on it to hold it to a stanchion," she said. "As I did so, three men pushed in front of me and shoved some screaming women out of the way. They went down the rope."
The fire burned intensely enough to heat the steel hull white-hot. Glass melted from portholes; metal slumped and warped. Enough water was poured in by the firefighting equipment to list the burning ship toward the dock; operations had to be halted until the list righted itself, as the Noronic settled to the bottom of the harbour with only her top decks above the surface. By five in the morning the fire was out, but they had to let the hull cool before venturing inside to find the bodies.
Everything that could be consumed inside the hull was consumed. Luxurious fittings were reduced to ash, ceilings and columns melted and warped. All the stairways in the boat save one were utterly destroyed.
The fire stripped away identities, turning human bodies to calcined bone fragments; some victims were nothing but a skull or spine. There are touchingly gruesome tales of searchers entering the ship to find embracing skeletons in the hallways and the remains of the cabins. The remains had to be removed by shoveling them onto tarpaulins, as they crumbled when picked up. New advances in forensic odontology (including the use of X-rays) had to be made to identify Noronic victims; articles on the techniques developed as a result of this disaster are still being published today in forensic journals.
Newspaper articles covering the disaster began, as newspaper articles of this sort tend to do, with horrified pronoun-deficient headlines: 200 DIE ON FIERY SHIP. GREAT LAKES QUEEN BURNS. HOLOCAUST SINKS PLEASURE CRUISER AT TORONTO DOCK. 400 HOLIDAYERS ESCAPE FLAMING DEATH AMID SCENES OF HORROR.
The final conclusion of the Court report into the disaster placed the blame on the failure of the owners and captain in:
a) Holding a continuous fire patrol of the ship, instead of a cursory time-clock round every 45 minutes
b) Maintaining any organized system while the ship was in dock with passengers aboard by which “information as to the outbreak of fire could be promptly dispatched to some point from which men trained in the methods of dealing with fire could be immediately dispatched to the locality,” or “effective fire alarm and fire procedure”
c) Taking the threat of fire at a dock seriously and allowing all but fifteen of the crew to go play on shore and be potentially unavailable in the case of emergency
d) Developing and practicing any plan for waking and evacuating passengers in the case of a fire while in dock
e) Training the crew on what to do in case of fire or how to operate the extinguishers and hoses.
Or, to put it more baldly, being about as prepared for a dockside fire as a jumbo prawn would be to handle a credit-default swap. The scope of the failure to prepare for or anticipate anything of the sort is breathtaking. The owners knew perfectly well that there was no functional plan in place for dealing with this kind of disaster, and so did the captain–and there was nothing stopping him from taking any steps to remedy the situation. It’s the equivalent of driving a car with half the lug nuts loose and just sort of hoping the damn wheels won’t come off.
The Noronic fire may not have been preventable, but the loss of life associated with it was. Nobody ever did determine what started it, but my money’s on an indifferently butted cigarette tossed into the refuse box in the linen closet, which then spread rapidly throughout a ship lacking in regulation fire-resistant bulkheads, a ship lined with highly inflammable varnished wood, a ship without automatic fire-detection or sprinkler systems, a ship whose fire alarm system was Goldbergian in its unnecessary complexity and multiple stages, and a ship manned by a totally insufficient and untrained skeleton staff. The bellboy O’Neill could possibly have saved the ship had he sounded the alarm before attempting to put the fire out himself–but he didn’t. The story of the Noronic is a litany of “I didn’t,” “I don’t know,” “I cannot say that I have,” and “I can’t see any reason why they would.”
Captain Taylor lost his license for a year; an unknown number of people lost their lives. The steamship company paid out something like $3 million to the families of the victims. Rather horribly, another Canadian passenger ship, the SS Quebec, experienced a similar fire a year later: the Quebec fire was ultimately determined to be the result of arson and started in a linen locker. None of the safety regulations written after Noronic were put in place aboard Quebec, and the crew were just about as useless in trying to fight the fire and evacuate passengers. That was it for Canada Steamship Lines’ passenger cruises on the Great Lakes.
It’s too easy to make fun of the Noronic’s name, which I will now reveal is most likely in reference to Lake Noron, Quebec. It’s too easy to point out that “no we didn’t” and “moronic” overlap quite efficiently, so I will just leave you with First Officer Wood’s deathless turn of phrase:
“I think in cases of emergency, the officer goes where he can be the best help.”
In this case, over the side.
Information in this article is taken from the following sources:
CanadianHistory.suite101.com
www.centrenaufrages.ca, Courage Tales 5, accessed June 16, 2009
GenDisasters.com
Lost Liners
Report of Court of Investigation into the Circumstances Attending the Loss of the S.S. "Noronic" (1949), located at Tales of Tragedy and Triumph: Canadian Shipwrecks, a virtual museum exhibition at Library and Archives Canada
The Walkerville Times
Wiki
The official "Report of Court of Investigation into the Circumstances Attending the Loss of the S.S. Noronic" contains quite a lot of direct quotes from examination of the various officers, included into the narrative to make the point abundantly clear: there was no official instruction given to crew members regarding their duties in case of fire in dock, and no attempts made to develop or distribute same, because “the ship had been running from 1913 without mishap.”
The Noronic, built (as mentioned) in 1913, was a cruise and package freight ship plying the Great Lakes. She had two sister ships, the Huronic and the Hamonic; this last, suffering under an even sillier name than Noronic, burned out in 1945. No apparent lessons were learned from the loss of the Hamonic, as demonstrated very clearly in the behaviour of the Noronic’s crew prior to and during the disaster.
She was vast for the time, capable of carrying six hundred passengers and two hundred crew on her five decks, and considered one of the most beautiful and luxurious cruise liners in Canada. Part of her luxury came from the fact that her interior walls were paneled in beautifully polished wood, into which thirty years of lovingly applied lemon-oil varnish had soaked. Some of the wood (the passenger accommodations on D deck) was painted rather than varnished, but the majority of the walls in the upper decks and communal areas were treated with this highly flammable oil.
She was also, being built prior to regulations passed in 1939, lacking the requisite fire-resistant bulkheads the regulations called for. The Chairman of the Board of Steamship Inspection was allowed to exempt existing ships from compliance with the regulations where it was “impracticable or unreasonable” to retrofit the ship to comply. In this case it was rather obviously “expensive” to do so, and Noronic remained a totally period-accurate vessel.
The series of legal loopholes through which the Noronic sailed to escape the installation of vital safety systems is impressive. Not only was she allowed to go around without fire-resistant bulkheads, she also did not have to comply with Regulation 3 of section 405 (1) c of the Canada Shipping Act, requiring “every ship…which is engaged on an international voyage, [to be provided with] an approved fire alarm or fire-detecting system which will automatically register at one or more points or stations in the ship, where it can be most quickly observed by officers and crew, the presence or indication of fire in any part of the ship…not accessible to a fire patrol system.”
Fire patrol meant that the crew was detailed to regularly make exhaustive rounds of the ship throughout the day and night to catch any hint of fire on board; the regulations stated that “all spaces in a passenger ship, except such spaces as cargo spaces, baggage and store rooms, may as a general rule be regarded as accessible to the patrol,” thereby exempting them from the requirement that an automatic alarm or detection system be fitted. Noronic was not considered international, as she only puttered around on the Great Lakes—an “inland voyage.” Even had she been considered “international” due to her route between Canada and the States and thus required to comply with Regulation 3, the Board of Steamship Inspection ruled in 1938 that Regulation 3 only applied to ships making international voyages on the ocean. Either it didn’t apply, or it didn’t apply.
Noronic did in fact have a manual fire alarm system that ran off batteries, of the in-case-of-fire-break-glass type. This alarm rang bells located a) in the officers’ quarters, b) on the port side of D deck, and c) in the engine room on E deck, registering the location of the pulled alarm. It did not activate the klaxons located around the ship which would alert passengers and crew to an emergency: in order to sound those someone would have to go up to the pilot house above A deck to manually flip the klaxon switch. The first and second officers informed investigators that it was “the duty of the officer on watch, upon hearing the bell alarm, to proceed to the locality from which the alarm had been given for the purpose of investigating whether the fire was serious enough to require the sounding of the klaxon alarm and, if he so concluded, then to return to the pilot hours above A deck where he would throw the switch which sounded the klaxon horns. If the officer on duty was away from the pilot house, the wheelsman who should be there was expected to find the officer on duty and report to him as to the locality at which the alarm had been sounded. To obtain this information he would first have to go to the bath-room in the mates’ quarters where the indicator was located.”
I quote the report again directly: It is, of course, obvious from the above that considerable time might be lost between the giving of the alarm at the point where the fire was first discovered and the giving of the klaxon alarm which could only be sounded from the pilot house.
No shit.
It goes on like that. There were supposed to be hydrants located all around the ship so that “at least two powerful jets of water can be rapidly and simultaneously brought to bear upon any part of each deck or space occupied by passengers or crew,” but the inspectors thought, eh, it’d be good enough if you could just run a hose down from the deck above if there weren’t enough hydrants on any given deck (even though the actual wording of the regulations states that “the hydrant shall be so placed on each deck that the fire hoses may be easily coupled to them").
It's apparent that nobody in a position to enforce safety regulations ever actually thought a fire could break out on the Noronic. Certainly they made every effort to weasel out of providing even the most basic of safety systems, taking advantage of the fact that as Noronic was merely sailing on a lake and not the ocean she did not strictly fall under the regulations requiring fire patrol. Whether this is due to some unknown dangerous quality in salt water as opposed to fresh is not explained. The report mentions tartly that in the judge’s opinion the regulations requiring ships to be equipped with working hydrants and extinguishers imply that there also should be crew members provided by the ship’s owner to use the aforementioned apparatus. Without an automatic fire detection system or a sprinkler system on board, Noronic really could’ve used a fire patrol. What they got was this:
Two crew members designated “Special Officers” switched off at 6-hour intervals to walk around the ship with a time clock and punch a series of keys located at various points on board “on the hour.”
Yeah. In 1942 Canada Steamship Lines issued a list of duties to be completed by the Special Officers, including:
“Each night from 9:00 PM until 6:00 AM the watchman clock shall be punched punctually on the hour. The dials are carefully checked by the Purser and the reason for not punching or the dials not being marked must be explained satisfactorily by the officer. During the round of punching, it is your duty to stop any excessive noise by passengers that are boisterous…Upon completion of your round and all passengers are quiet [sic], return to the rotunda where you are easily found should you be needed…”
The round of time-clock punching took about 15 minutes, which meant that for 45 minutes out of every hour there was pretty much zero fire patrol going on. One of Noronic’s Special Officers said that he thought he wasn’t supposed to do the patrol at all when the ship was in port, but remain instead at the gangplank; the other one understood his duty to be completing the rounds each hour and then returning to the gangplank. In fact neither of them were on board the night of the fire: both Special Officers’ rounds were conducted by a pair of wheelsmen who took the shortest possible routes between the time clocks.
This lack of clarity amongst officers and crew comes up over and over again throughout the investigation. This officer understood that this other officer was supposed to do something, but didn't check with anyone to see if this was in fact the case; that officer thought he was supposed to do this other thing but in point of fact was supposed to be somewhere else entirely and had no idea what to do in case of emergency. The card in the passengers' accommodations regarding fire stated confidently that the ship was equipped with "modern fire prevention apparatus" and patrolled "day and night by experienced watchmen." Or inexperienced wheelsmen doing the watchmen's jobs for them, either way.
Fire and lifeboat drills were regularly held on board the Noronic when she was moored in Duluth. Every Tuesday at ten in the morning, the signal was given for fire drill and the crew members assigned to "fire stations" (hydrants) gathered at their posts. The objective of the drill was to get to the hydrant, get the hose down from its rack, and couple the hose to the hydrant. Sometimes on the outside fire stations they'd squirt the hoses overboard, but obviously not indoors. A few crew members were expected to get the extinguishers down and wave them about, maybe discharge one or two. That was it for fire training of the crew.
In 1945, the General Manager at Canada Steamship Lines was apparently made aware of the fact that his ships were practicing a thoroughly useless excuse for a fire drill, and sent out a memo with an updated list of rules. The memo stated that the enclosed Lifeboat and Fire Drill Regulations were (I quote) serious business, and that masters of all passenger steamers must study them carefully and instruct all crew members accordingly. Let's see how the Norons did:
1) MUSTER STATIONS: The Master will designate locations of muster stations throughout the ship to which members of the crew will report for lifeboat and fire drills (and make sure all crew members know where these stations are and which signals call for them to muster).
1) a ALARM SIGNALS: General or Fire Alarm is indicated by one long, three short, one long blasts on whistle or alarm. Proceed at once to fire drill assigned station. Man Boats Alarm is indicated by General Alarm followed by two short blasts on whistle or alarm. Proceed at once to boat drill assigned station.
The Noronic's crew members each carried a blue card on which was printed his crew number, his fire station number, and his boat number. It clearly states the types of alarm and what one should do upon hearing them. However, in practice, the fire drill signal was a continuous blast on the klaxon horns, while the lifeboat drill signal was identical to the official "general or fire alarm" signal. Crew members had to learn to ignore the info on the blue card.
Passengers did not take part in either drill. The only information they received on what to do in case of fire was on the instruction cards in their rooms. The crew were the only ones who had any idea of emergency procedures, and their grasp on same was tenuous at best.
2) MUSTER LISTS: The Master will have a muster list prepared including the information of all crew members and their muster stations, as well as "full particulars" of the signals required to call members of the crew to muster. This list shall be posted in conspicuous places throughout the ship including the crew's quarters and every officer's room.
There was no such thing as a "muster list" on board the Noronic, nothing signed by the Master, and nothing hung in any officer's room. A "chart" of crew members apparently hung in the maids' quarters, in the crew's stairway aft, on either B or C decks, and in the crew's rec room. The first officer, Gerald Wood, used this chart to prepare a list of crew members and their blue card numbers, boat numbers, and hydrant numbers, and gave a copy to the chief steward. The captain was completely ignorant of all of this and only knew about the typed list because he looked over Wood's shoulder as he was filling it out. Who's on board? Whose job is it to do what? Who knows?
3) MUSTER CARDS: A card indicating the muster station for each crew member must be placed in his berth in such position that it cannot be obscured by baggage or clothing.
The only thing remotely similar to this in use on the Noronic was the blue card, which was kept wherever the crew felt like keeping it.
There was also a rule stating that the Master had to appoint Senior Officers to various parts of the ship in order to help direct passengers to their muster stations if necessary. Here is where the testimony really gets interesting: Captain Taylor said that he'd allocated the first officer to C deck, second officer to A deck, third officer to B deck, and chief steward and purser to D deck. Wood, the first officer, denies any allocation was made, and then proceeds to flip-flop like a gaffed pike (unsurprisingly, he stated that he had never seen or heard of the Serious Business memo):
Q: Was there any allocation that you know of of senior officers allocated to certain locations for the purpose of mustering passengers?
A: No there was not.
Q: Did you make any allocation?
A: No.
Q: Did anyone else to your knowledge?
A: Not that I know of.
Q (really trying here): Now I want to be fair with you. I thought the Captain did say to us that he had allocated certain senior officers in accordance with this and he said the allocation was the chief officer to C deck....do you know anything about that?
A: Well yes, I would be in charge of C deck.
Q: (wondering what he's smoking): Well that is what he told us, that you were in charge of C deck--then must that not mean that you were allocated in some way to C deck?
A: Yes, I would be allocated.
Q: How would you be allocated and what instructions did you have with regard to C deck?
A: I think by this chart [which indicated his duty was free to move about the ship].
(some back and forth about whether or not this allocation is the same as on other ships)
Q: Now what do you say as to whether or not any station was allocated to you as the first officer under this regulation?
A: Well he may have told me to go to my allocation on C deck.
Q: (between clenched teeth) Well he may and then I suppose he may not, but I am trying to get from you whether he did.
A: Well I have been there a number of years.
Q: Then is your statement to me that you do not know whether the Captain in the case of fire had told you that you were to go to C deck?
A: I am pretty sure--I might say that the captain did not tell me this year. He could have back in 1944 or 1945.
Q: Did you always go to C deck on fire drill?
A: No, I go all over the ship.
Q: Then you were really not allocated to C deck?
A: Not to stay there.
Q: Well was anybody allocated to C deck?
A: Well I think the officers were free--wherever we could be the most help.
This confusion is heightened by "the chart," which states that Wood was in fact in charge of deck A. Balancing out various testimonies against one another it becomes abundantly clear that this "chart" had become so obsolete by 1949 that it had nothing to do with any organization or lack thereof on board the ship and in fact the captain had no idea it existed at all. We are dealing with governmental levels of confusion here. The captain and first officer, when asked about duties to be performed by the officers and men at the fire hydrant stations, contradicted one another and made up answers to explain what the rest of the crew not assigned to hydrants would be doing (running away, is my guess).
The slipperiness of officials when faced with questions about the Noronic extends way up the ladder. General Manager of the line Captain Reoch had to admit under examination that in fact when he wrote the Serious Business memo he did not take into consideration the fact that, if a fire occurred while the ship was tied up to a dock, directing all the passengers to the muster stations on C deck would not do them a blind bit of good as the only gangplanks to the dock were on E deck three floors below. "Was it your intention under these rules when you drew them up, that in the event of a fire at a dock, the passengers from D deck would go up or be directed to C deck and then go back down to D [and then E] deck to get off onto the dock?" he was asked. After some squirming and repeated requests to answer the question, Reoch finally admitted that he didn't think that the rules he'd indicated would be followed in case of a dockside fire--or, more accurately, he'd not bothered to consider the possibility.
The really damning bit is when they are asked why they didn't increase the number of crewmen on fire patrol while the ship was tied up. "If there had of [sic] been any signs of an emergency, yes, but there was no reason why they would have. I can't see any reason why they would."
Maybe because you're in a floating firetrap lacking rudimentary safety systems, steeped in decades' worth of flammable varnish, and inhabited by people who are coming back from Toronto bars drunk off their tits and probably waving around lit cigars?
There was no way of knowing which crew members were on or off the ship while she was in port, as they were free to go ashore at any time they were not on duty. If there had been any organization amongst the crew for dealing with emergencies, it went directly out of the porthole as soon as crew members began to go ashore unremarked.
So we have the perfect setup for disaster. On the night of September 17, 1949, something in a linen closet on C deck aft caught fire. The closet contained bed linen, towels, and cleaning materials, as well as a box for rubbish and wastepaper collected from the cabins, and a switchbox controlling some of the stateroom lights. The presence of the box is controversial: a maid stated that the rubbish box was never placed in the linen closet; the chief steward said it might have been there, and an eyewitness stated that it was there. If the fire was due to a smouldering cigarette butt, this box would have represented a perfect point of origin. Passengers mentioned seeing maids smoking cigarettes in the linen closet during the voyage; in the absence of a major electrical fault it seems likely although not certain that a carelessly discarded butt was responsible for killing somewhere between 118 and 139 people.
A passenger, Don Church, noticed a haze in the starboard corridor around 2:30 a.m. and followed it to the linen closet, where he saw smoke coming from the sides and top of the locked closet door. He heard a faint crackling, rustling noise, and assumed someone was inside; this would have been the fire talking to itself. Church, unable to open the door, ran forward yelling that the boat was on fire and encountered the head bellboy, Earnest O'Neill. O'Neill ran back with him to the locker, whereupon their stories diverge: O'Neill stated that he ran back to the steward's officers to fetch the closet key, then went to fetch a fire extinguisher before unlocking the door. Church stated that he just unlocked the door as they arrived.
They opened the door and saw that the wall was in flames and a hanging sheet was beginning to burn. The extinguisher barely slowed it down: almost as soon as the door was opened, flames poured out along the ceiling, feeding on the beautifully polished wooden paneling. Church and O'Neill went for a fire hose, but when Church opened the valve nothing came out. At this point he thought sod this for a game of soldiers and went off to fetch his family and got the hell out of it.
O'Neill only now broke the glass on the fire alarm and ran down to E deck to find a wheelsman and inform him of the fire. It's uncertain how much time really elapsed between the discovery of the fire and the sounding of the alarm, but time was definitely lost in trying to put out the fire with ineffective means. If O'Neill had sounded the alarm at once instead of messing about with extinguishers, several senior officers could have responded at once and taken charge of the fire equipment: C deck was the most well-staffed in terms of hydrant stations. He didn't. The fire raged out of control.
The wheelman O'Neill had woken in turn woke Wood, who quickly sounded the klaxon alarm and pulled the whistle, which stuck open and drowned out the klaxons. By now the starboard side of the boat was "full of fire," and he could not go aft farther than the first three cabins on the port side, where he "banged on the windows" and shouted.
Just before Wood sounded the whistle, a night watchman on the pier was appalled to see flames breaking through a window on the ship's starboard side. He ran inside and called the fire department and gave the alarm, then called the police; someone else standing at the door told him to call for ambulances as well. After he'd told the police to send all the doctors and ambulances they could, the watchman--a Mr. Harper--went back outside to find a mass of flame engulfing the starboard side of the ship. Now the whistle was blowing--Wood had sounded the alarm--and the fire department was arriving. By now it was 2:41 a.m., eleven minutes since Church first saw the smoke, and half the ship's decks were on fire.
The man who had told Harper to call for ambulances was one of the first to escape the burning ship. He had seen people badly burned--a woman with her hair burned away, people with faces and arms scorched and bubbling. It was still only minutes after the fire had begun, and already it was lethal.
The captain was informed of the fire some time between 2:30 and 2:35, according to his testimony, but the times don't match up; he claims to have gone out to yell for help from the outside deck and observed people on the pier, but Harper the watchman had seen the fire begin to erupt and made the alarm call when there had been no other people on the dock.
There is considerable flip-flopping from Wood regarding the instructions he had given to the crew members as to what they ought to do in case of fire: should they notify the officer on watch or just any officer, should they use a hose or an extinguisher first, did he actually tell them anything at all. "Would this be fair," he was asked, "and now correct me if I do not say it correctly--that so far as the education of the crew in the event of fire was concerned, all they had was what they saw on the printed chart in the crew's quarters, which took them to their various stations in the event of hearing the alarm--is that all they had--apart from what you have just said as to what you might have told any particular member of the crew--does that cover the whole field?"
"Yes, that covers it."
There was no organization, and therefore there was no clear and evident list of duties for each member of the crew to perform. Some of the fifteen men on duty tried harder than others to waken passengers and shepherd them over the side on ropes and Jacob's-ladders; by now the fire department was there en masse and trying to reach the ship with aerial ladders, but so many people leapt on the first of these--Aerial No. 5--that it snapped and spilled the lot of them into the harbour. Other passengers leapt straight into the water, some of them screaming as they burned, some of them in eerie silence. Many people were asleep when the fire broke out, and woke only to find their cabins ablaze and the only way out blocked by a window-screen they could not break; some were pulled from burning cabins from the outside by crew members or fellow passengers who had broken the screens away.
GenDisasters offers a collection of quotes from eyewitnesses. Mildred Briggs of Detroit, one of the survivors, said the flames spread as if in a matchbox. "The fire just welled up along the corridors and spread faster than any fire I've ever seen," she said.
"There was a mob of men and women surging back and forth," said another survivor, Alberta Agia of Detroit. "Men were pushing women around, and many were knocked to the floor. The screaming filled the air. There was so much panic that I don't know how these people found anyway to safety. I slid down a rope."
Men rushed out in their nightclothes. One man got ashore naked.
Henry Maurer and his wife were sound asleep when someone pounded the door. When they reached the outside rail, his wife started down a rope ladder, "but it became horribly twisted from so many trying to get on it. She got tangled and trapped. I swung down on a rope to her side and got her free, and we both managed to get to the dock."
Sylvia Carpenter of Detroit said she screamed and headed for the outside rail when she saw smoke and flame billowing along the passageways.
"A rope was tossed over the rail and I put a hitch knot on it to hold it to a stanchion," she said. "As I did so, three men pushed in front of me and shoved some screaming women out of the way. They went down the rope."
The fire burned intensely enough to heat the steel hull white-hot. Glass melted from portholes; metal slumped and warped. Enough water was poured in by the firefighting equipment to list the burning ship toward the dock; operations had to be halted until the list righted itself, as the Noronic settled to the bottom of the harbour with only her top decks above the surface. By five in the morning the fire was out, but they had to let the hull cool before venturing inside to find the bodies.
Everything that could be consumed inside the hull was consumed. Luxurious fittings were reduced to ash, ceilings and columns melted and warped. All the stairways in the boat save one were utterly destroyed.
{kind=link}
{kind=link}
The fire stripped away identities, turning human bodies to calcined bone fragments; some victims were nothing but a skull or spine. There are touchingly gruesome tales of searchers entering the ship to find embracing skeletons in the hallways and the remains of the cabins. The remains had to be removed by shoveling them onto tarpaulins, as they crumbled when picked up. New advances in forensic odontology (including the use of X-rays) had to be made to identify Noronic victims; articles on the techniques developed as a result of this disaster are still being published today in forensic journals.
Newspaper articles covering the disaster began, as newspaper articles of this sort tend to do, with horrified pronoun-deficient headlines: 200 DIE ON FIERY SHIP. GREAT LAKES QUEEN BURNS. HOLOCAUST SINKS PLEASURE CRUISER AT TORONTO DOCK. 400 HOLIDAYERS ESCAPE FLAMING DEATH AMID SCENES OF HORROR.
The final conclusion of the Court report into the disaster placed the blame on the failure of the owners and captain in:
a) Holding a continuous fire patrol of the ship, instead of a cursory time-clock round every 45 minutes
b) Maintaining any organized system while the ship was in dock with passengers aboard by which “information as to the outbreak of fire could be promptly dispatched to some point from which men trained in the methods of dealing with fire could be immediately dispatched to the locality,” or “effective fire alarm and fire procedure”
c) Taking the threat of fire at a dock seriously and allowing all but fifteen of the crew to go play on shore and be potentially unavailable in the case of emergency
d) Developing and practicing any plan for waking and evacuating passengers in the case of a fire while in dock
e) Training the crew on what to do in case of fire or how to operate the extinguishers and hoses.
Or, to put it more baldly, being about as prepared for a dockside fire as a jumbo prawn would be to handle a credit-default swap. The scope of the failure to prepare for or anticipate anything of the sort is breathtaking. The owners knew perfectly well that there was no functional plan in place for dealing with this kind of disaster, and so did the captain–and there was nothing stopping him from taking any steps to remedy the situation. It’s the equivalent of driving a car with half the lug nuts loose and just sort of hoping the damn wheels won’t come off.
The Noronic fire may not have been preventable, but the loss of life associated with it was. Nobody ever did determine what started it, but my money’s on an indifferently butted cigarette tossed into the refuse box in the linen closet, which then spread rapidly throughout a ship lacking in regulation fire-resistant bulkheads, a ship lined with highly inflammable varnished wood, a ship without automatic fire-detection or sprinkler systems, a ship whose fire alarm system was Goldbergian in its unnecessary complexity and multiple stages, and a ship manned by a totally insufficient and untrained skeleton staff. The bellboy O’Neill could possibly have saved the ship had he sounded the alarm before attempting to put the fire out himself–but he didn’t. The story of the Noronic is a litany of “I didn’t,” “I don’t know,” “I cannot say that I have,” and “I can’t see any reason why they would.”
Captain Taylor lost his license for a year; an unknown number of people lost their lives. The steamship company paid out something like $3 million to the families of the victims. Rather horribly, another Canadian passenger ship, the SS Quebec, experienced a similar fire a year later: the Quebec fire was ultimately determined to be the result of arson and started in a linen locker. None of the safety regulations written after Noronic were put in place aboard Quebec, and the crew were just about as useless in trying to fight the fire and evacuate passengers. That was it for Canada Steamship Lines’ passenger cruises on the Great Lakes.
It’s too easy to make fun of the Noronic’s name, which I will now reveal is most likely in reference to Lake Noron, Quebec. It’s too easy to point out that “no we didn’t” and “moronic” overlap quite efficiently, so I will just leave you with First Officer Wood’s deathless turn of phrase:
“I think in cases of emergency, the officer goes where he can be the best help.”
In this case, over the side.
Information in this article is taken from the following sources:
CanadianHistory.suite101.com
www.centrenaufrages.ca, Courage Tales 5, accessed June 16, 2009
GenDisasters.com
Lost Liners
Report of Court of Investigation into the Circumstances Attending the Loss of the S.S. "Noronic" (1949), located at Tales of Tragedy and Triumph: Canadian Shipwrecks, a virtual museum exhibition at Library and Archives Canada
The Walkerville Times
Wiki
Friday, June 12, 2009
I love the smell of corporate negligence in the morning: the Boston Molasses Flood
Clichés tend to become clichés for a reason. “Slow as molasses” is generally an apt statement: molasses is highly viscous and therefore flows at a slow rate of speed. Comparing something slow to the movement of molasses is valid.
Except when the molasses is going thirty-five miles an hour.
Ninety years ago, Boston’s North End was the home of the city’s busiest center of commerce: the North End Paving Yard and the Commercial Street Wharf. Freighters from all over the world crowded against one another, taking on or discharging cargoes–livestock, tea, coffee, wool, raw materials for a hundred different trades; locomotives shunted freight cars to and from the wharf to deliver or receive goods from the ships. Stonecutters chipped and shaped pavement blocks in the Yard. Successive waves of immigrants had settled in the neighborhood, and the patter of stevedores and dockhands and blacksmiths and drivers varied from Italian to Irish. There was a lot of work to be had, and a lot of workers competing for it.
One of the landmarks of the North End waterfront was the United States Industrial Alcohol Company’s fifty-foot-high storage tank, holding the molasses the company used to distill its product. This tank, capable of holding over two million gallons of molasses, was used to store molasses from freight tankers before discharging it to railway tank cars for transportation to USIA’s distillation plant. It had been built in a tearing hurry during the month of December, 1915, after lengthy delays in negotiation regarding leasing the land for the tank site and securing permission for the construction. USIA needed the tank ready to accept a shipment of molasses by December 31, and by jingo it was completed in time.
It wasn’t tested to see how the construction held up, of course, because it would have taken days and dollars to fill it up with water: the individual responsible for the construction of the tank, Arthur P. Jell, happened to be the treasurer of USIA’s subsidiary Purity Distilling, and was well aware of the amount the company stood to lose if they wasted any time. Jell instructed that the tank should be filled with water to the level of six inches, enough to cover the joint at the base of the construction, and when this did not result in leaks he declared the tank safe for use.
In point of fact it leaked like an enuretic hamster. In February 1916, two months after completion, the tank was observed to be leaking molasses from its seams, dribbling the stuff in slow streams down the outside to pool around the base in quantities sufficient for children to come and scoop it up in pails. The leaks had been reported to the company, and Jell ordered the tank recaulked twice and painted brown to hide the leaks.
Stephen Puleo’s comprehensive book on the disaster, The Dark Tide, describes one employee, Isaac Gonzalez, as feeling the tank vibrate and hearing it groan every time a shipment of molasses was pumped in. According to Puleo, Gonzalez was deeply concerned about the tank’s structural integrity, and when he was warned after mentioning the leakage that voicing further complaints or concerns to management would get him fired, he took it upon himself to do what he could to lower the risk of disaster. This included sleeping in an office next to the tank so as to be able to sound an alarm in case of imminent rupture. On one of the nights he spent in the office by the tank, he received an anonymous phone call stating that the tank would be blown up with dynamite and everyone who worked there would be killed.
This last was more of a worrisome threat than might be imagined. At the time, USIA’s ethanol was being used in manufacturing munitions for the war in Europe; it was thought that the anti-war anarchists who had been operating in the area might target the plant. After that phone call Gonzalez no longer slept by the tank; however, Puleo’s book offers a vivid description of his nightly visits to the plant to secretly release molasses into the harbor and ease the pressure within the tank:
Working quickly, Isaac twisted open a valve and began releasing molasses into the harbor, and along with it any gasses that had built up inside the tank. After ten minutes, he closed and tightened the valve. He had no idea how many gallons of molasses had been dumped, and practically speaking knew it would make little difference in the overall capacity of the tank, which held over two million gallons when it was full. Isaac also knew that he would be fired, prosecuted, and most likely sent to jail if Mr. Jell ever found out about these late-night visits. But dumping the molasses helped clear his head and made him feel less helpless. (Puleo, p.5)
Over the next two years the tank continued to dribble molasses and make alarming groaning noises when the supply was pumped in, but nothing more. Most likely no single factor can be blamed for its disastrous failure: a combination of shoddy and rapid construction, lack of maintenance or safety oversight, freak temperature changes, and general bad luck was probably responsible.
The temperature on the 15th was forty-three degrees Fahrenheit, unseasonably warm for January; on the 12th it had been two degrees, on the 13th sixteen, and on the 14th it had jumped from sixteen to forty. Fermentation may have taken place within the tank as the temperature rose sharply, producing carbon dioxide and increasing the tank’s internal pressure beyond its structural limits. Whatever was responsible, the result was the same.
Half past noon on Wednesday, January 15, a low rumbling noise like a train passing by shook the ground, accompanied by a rapid staccato machine-gun roar as the tank rivets shot away from their plates and the bottom of the massive tank ruptured, spewing out approximately 2,300,000 gallons of molasses. The force of the escaping fluid split the remains of the tank in half.
In a 1965 article originally printed in Yankee Magazine, John Mason describes the first moments of the disaster:
[In] less time than it takes to tell it, molasses had filled the five-foot loading pit, and was creeping over the threshold of the warehouse door. The four loaded freight cars were washed like chips down the track. The half-loaded car was caught on the foaming crest of the eight-foot wave and, with unbelievable force, hurled through the corrugated iron walls of the terminal.
The freight house shook and shivered as the molasses outside, now five feet deep, pushed against the building. Then the doors and windows caved in, and a rushing-roaring river of molasses rolled like molten lava into the freight shed, knocking over the booths where freight clerks were checking their lists.
Like madmen they fought the on-rushing tide, trying to swim in the sticky stuff that sucked them down. Tons of freight—shoes, potatoes—barrels and boxes—tumbled and splashed on the frothy-foaming mass, now so heavy the floors gave way, letting tons of the stuff into the cellar. Down there the workers died like rats in a trap. Some tried to dash up the stairs but they slipped and fell—and disappeared.
As the fifty-eight-foot-high tank split wide open, more molasses poured out under a pressure of two tons per square foot. Men, women, children and animals were caught, hurled into the air, or dashed against freight cars only to fall back and sink from sight in the slowly moving mass.
Having wiped the freight house off the face of the Earth, the molasses lahar proceeded to take out part of the El support, destroying a section of track, knocked over a fire station, filled up a Public Works building, and turned a number of houses into gluey matchwood, moving at an estimated thirty-five miles per hour.* Twenty-one people died, either crushed to death or drowned in molasses–which if you stop to think about it is a peculiarly horrible way to die–and a hundred and fifty more were injured in the disaster. Two of the dead could not be identified, too battered and candied for recognition.
Unlike floods of, say, water, the molasses flood’s clean-up took weeks. Squirting water on the ankle-deep goo did nothing at all; firemen eventually had to use salt water to blast molasses from the streets and walls, washing it down into the harbor (which was brown and redolent of sugar for months). It took 87,000 man-hours to clean up the mess, and a further six years before the ensuing trial was completed and a report published. USIA, unsurprisingly, was found responsible for the disaster through an insufficient “factor of safety,” meaning they didn’t build the damn tank strong enough to hold its contents. Which Isaac Gonzalez pointed out to Arthur Jell in 1915.
Today the site of the tank has been turned into a playground, next to a park; there’s a small plaque at the entrance to the park commemorating the flood:
On January 15, 1919, a molasses tank at 529 Commercial Street exploded under pressure, killing 21 people. A 40-foot wave of molasses buckled the elevated railroad tracks, crushed buildings and inundated the neighborhood. Structural defects in the tank combined with unseasonably warm temperatures contributed to the disaster.
They say that on hot days you can still smell ninety-year-old molasses in the air. It’s still there, of course, in the joints between bricks, in the ground, in the earth. It’s the sweet smell of criminal negligence–less sickly than trichloroethylene, but no less accusatory.
* Cecil Adams of The Straight Dope discusses the speed of the flow (note that Adams apparently supports the conspiracy theory that USIA decided to fill up the tank to distill molasses into grain alcohol for liquor before Prohibition killed the market for good):
I consulted with Gareth McKinley, professor of mechanical engineering at MIT, and established that the theoretical maximum rate of flow for a (roughly) 50-foot column of liquid, ignoring density and viscosity, was 38 mph. Surprisingly, molasses's stiffness would have slowed things only a bit--making certain assumptions about Reynolds number and whatnot that I expect some gratitude for not sharing, the flow rate would have been mostly a function of inertia (i.e., mass) rather than viscosity. Bottom line: 35 mph was a pretty good guess.
Information in this article was taken from the following:
John Mason, “Eric Postpischil's Molasses Disaster Pages, Yankee Magazine Article,” Eric Postpischil's Domain, 29 August 2007, accessed 12 June 2009
Edwards Park, “Eric Postpischil's Molasses Disaster Pages, Smithsonian Article,” Eric Postpischil's Domain, 29 August 2007, accessed 12 June 2009
Puleo, Stephen, "Dark Tide: The Great Boston Molasses Flood of 1919". Beacon Press, 2004, preview available at Google Books
and of course
Wiki
Except when the molasses is going thirty-five miles an hour.
Ninety years ago, Boston’s North End was the home of the city’s busiest center of commerce: the North End Paving Yard and the Commercial Street Wharf. Freighters from all over the world crowded against one another, taking on or discharging cargoes–livestock, tea, coffee, wool, raw materials for a hundred different trades; locomotives shunted freight cars to and from the wharf to deliver or receive goods from the ships. Stonecutters chipped and shaped pavement blocks in the Yard. Successive waves of immigrants had settled in the neighborhood, and the patter of stevedores and dockhands and blacksmiths and drivers varied from Italian to Irish. There was a lot of work to be had, and a lot of workers competing for it.
One of the landmarks of the North End waterfront was the United States Industrial Alcohol Company’s fifty-foot-high storage tank, holding the molasses the company used to distill its product. This tank, capable of holding over two million gallons of molasses, was used to store molasses from freight tankers before discharging it to railway tank cars for transportation to USIA’s distillation plant. It had been built in a tearing hurry during the month of December, 1915, after lengthy delays in negotiation regarding leasing the land for the tank site and securing permission for the construction. USIA needed the tank ready to accept a shipment of molasses by December 31, and by jingo it was completed in time.
It wasn’t tested to see how the construction held up, of course, because it would have taken days and dollars to fill it up with water: the individual responsible for the construction of the tank, Arthur P. Jell, happened to be the treasurer of USIA’s subsidiary Purity Distilling, and was well aware of the amount the company stood to lose if they wasted any time. Jell instructed that the tank should be filled with water to the level of six inches, enough to cover the joint at the base of the construction, and when this did not result in leaks he declared the tank safe for use.
In point of fact it leaked like an enuretic hamster. In February 1916, two months after completion, the tank was observed to be leaking molasses from its seams, dribbling the stuff in slow streams down the outside to pool around the base in quantities sufficient for children to come and scoop it up in pails. The leaks had been reported to the company, and Jell ordered the tank recaulked twice and painted brown to hide the leaks.
Stephen Puleo’s comprehensive book on the disaster, The Dark Tide, describes one employee, Isaac Gonzalez, as feeling the tank vibrate and hearing it groan every time a shipment of molasses was pumped in. According to Puleo, Gonzalez was deeply concerned about the tank’s structural integrity, and when he was warned after mentioning the leakage that voicing further complaints or concerns to management would get him fired, he took it upon himself to do what he could to lower the risk of disaster. This included sleeping in an office next to the tank so as to be able to sound an alarm in case of imminent rupture. On one of the nights he spent in the office by the tank, he received an anonymous phone call stating that the tank would be blown up with dynamite and everyone who worked there would be killed.
This last was more of a worrisome threat than might be imagined. At the time, USIA’s ethanol was being used in manufacturing munitions for the war in Europe; it was thought that the anti-war anarchists who had been operating in the area might target the plant. After that phone call Gonzalez no longer slept by the tank; however, Puleo’s book offers a vivid description of his nightly visits to the plant to secretly release molasses into the harbor and ease the pressure within the tank:
Working quickly, Isaac twisted open a valve and began releasing molasses into the harbor, and along with it any gasses that had built up inside the tank. After ten minutes, he closed and tightened the valve. He had no idea how many gallons of molasses had been dumped, and practically speaking knew it would make little difference in the overall capacity of the tank, which held over two million gallons when it was full. Isaac also knew that he would be fired, prosecuted, and most likely sent to jail if Mr. Jell ever found out about these late-night visits. But dumping the molasses helped clear his head and made him feel less helpless. (Puleo, p.5)
Over the next two years the tank continued to dribble molasses and make alarming groaning noises when the supply was pumped in, but nothing more. Most likely no single factor can be blamed for its disastrous failure: a combination of shoddy and rapid construction, lack of maintenance or safety oversight, freak temperature changes, and general bad luck was probably responsible.
The temperature on the 15th was forty-three degrees Fahrenheit, unseasonably warm for January; on the 12th it had been two degrees, on the 13th sixteen, and on the 14th it had jumped from sixteen to forty. Fermentation may have taken place within the tank as the temperature rose sharply, producing carbon dioxide and increasing the tank’s internal pressure beyond its structural limits. Whatever was responsible, the result was the same.
Half past noon on Wednesday, January 15, a low rumbling noise like a train passing by shook the ground, accompanied by a rapid staccato machine-gun roar as the tank rivets shot away from their plates and the bottom of the massive tank ruptured, spewing out approximately 2,300,000 gallons of molasses. The force of the escaping fluid split the remains of the tank in half.
In a 1965 article originally printed in Yankee Magazine, John Mason describes the first moments of the disaster:
[In] less time than it takes to tell it, molasses had filled the five-foot loading pit, and was creeping over the threshold of the warehouse door. The four loaded freight cars were washed like chips down the track. The half-loaded car was caught on the foaming crest of the eight-foot wave and, with unbelievable force, hurled through the corrugated iron walls of the terminal.
The freight house shook and shivered as the molasses outside, now five feet deep, pushed against the building. Then the doors and windows caved in, and a rushing-roaring river of molasses rolled like molten lava into the freight shed, knocking over the booths where freight clerks were checking their lists.
Like madmen they fought the on-rushing tide, trying to swim in the sticky stuff that sucked them down. Tons of freight—shoes, potatoes—barrels and boxes—tumbled and splashed on the frothy-foaming mass, now so heavy the floors gave way, letting tons of the stuff into the cellar. Down there the workers died like rats in a trap. Some tried to dash up the stairs but they slipped and fell—and disappeared.
As the fifty-eight-foot-high tank split wide open, more molasses poured out under a pressure of two tons per square foot. Men, women, children and animals were caught, hurled into the air, or dashed against freight cars only to fall back and sink from sight in the slowly moving mass.
Having wiped the freight house off the face of the Earth, the molasses lahar proceeded to take out part of the El support, destroying a section of track, knocked over a fire station, filled up a Public Works building, and turned a number of houses into gluey matchwood, moving at an estimated thirty-five miles per hour.* Twenty-one people died, either crushed to death or drowned in molasses–which if you stop to think about it is a peculiarly horrible way to die–and a hundred and fifty more were injured in the disaster. Two of the dead could not be identified, too battered and candied for recognition.
Unlike floods of, say, water, the molasses flood’s clean-up took weeks. Squirting water on the ankle-deep goo did nothing at all; firemen eventually had to use salt water to blast molasses from the streets and walls, washing it down into the harbor (which was brown and redolent of sugar for months). It took 87,000 man-hours to clean up the mess, and a further six years before the ensuing trial was completed and a report published. USIA, unsurprisingly, was found responsible for the disaster through an insufficient “factor of safety,” meaning they didn’t build the damn tank strong enough to hold its contents. Which Isaac Gonzalez pointed out to Arthur Jell in 1915.
Today the site of the tank has been turned into a playground, next to a park; there’s a small plaque at the entrance to the park commemorating the flood:
On January 15, 1919, a molasses tank at 529 Commercial Street exploded under pressure, killing 21 people. A 40-foot wave of molasses buckled the elevated railroad tracks, crushed buildings and inundated the neighborhood. Structural defects in the tank combined with unseasonably warm temperatures contributed to the disaster.
They say that on hot days you can still smell ninety-year-old molasses in the air. It’s still there, of course, in the joints between bricks, in the ground, in the earth. It’s the sweet smell of criminal negligence–less sickly than trichloroethylene, but no less accusatory.
* Cecil Adams of The Straight Dope discusses the speed of the flow (note that Adams apparently supports the conspiracy theory that USIA decided to fill up the tank to distill molasses into grain alcohol for liquor before Prohibition killed the market for good):
I consulted with Gareth McKinley, professor of mechanical engineering at MIT, and established that the theoretical maximum rate of flow for a (roughly) 50-foot column of liquid, ignoring density and viscosity, was 38 mph. Surprisingly, molasses's stiffness would have slowed things only a bit--making certain assumptions about Reynolds number and whatnot that I expect some gratitude for not sharing, the flow rate would have been mostly a function of inertia (i.e., mass) rather than viscosity. Bottom line: 35 mph was a pretty good guess.
Information in this article was taken from the following:
John Mason, “Eric Postpischil's Molasses Disaster Pages, Yankee Magazine Article,” Eric Postpischil's Domain, 29 August 2007, accessed 12 June 2009
Edwards Park, “Eric Postpischil's Molasses Disaster Pages, Smithsonian Article,” Eric Postpischil's Domain, 29 August 2007, accessed 12 June 2009
Puleo, Stephen, "Dark Tide: The Great Boston Molasses Flood of 1919". Beacon Press, 2004, preview available at Google Books
and of course
Wiki
Thursday, June 11, 2009
Lake Peigneur: d’oh on a scale that’s hard to imagine
Think about salt for a moment. In recent years it’s gone from the standard fine-crystal iodized stuff that came in cardboard canisters and was not generally considered a subject for rhapsody to a whole new world of artisanal seasonings: much like bread, salt has become fashionable, and salt snots now argue with one another over the relative benefits of flake salt, fleur du sel, French grey salt, Hawaiian pink salt, or Indian black salt (“an unrefined mineral salt. It is actually a pearly pinkish gray rather than black, and has a strong, sulfuric flavor. Uses: Use in authentic Indian cooking”).
Before there was saltnews.com, you got your salt from industrial salt mines. Rock salt, or halite, the stuff that rots the undercarriage of your car in winter, represents ancient salt deposited in marine basins as water evapourated. Over time, the salt beds were covered with layers of sediment and compressed. Salt is less dense than the surrounding rock, and it has a tendency to push upward in blobby formations called salt domes (topographical modeling of these formations looks a lot like the bottom of a lava lamp as it warms up). These domes can be absolutely massive, shouldering aside mountains as they bubble to the surface.
As the salt domes squash and displace strata around and above them, pockets are formed between salt and rock where oil and natural gas can collect. Salt mining operations, therefore, are often found right next to oil/gas drilling operations–including under the Gulf Coast. Mostly this does not present a problem. Mostly.
Imagine a salt mine that is busily chipping away at a salt dome that happens to be directly under a shallow lake. The miners know perfectly well where they can and cannot dig; the tunnels extend far below the lake itself, and the mine is producing a healthy crop of salt for the Diamond Crystal Salt Company. It’s November 21, 1980, and the most bizarre man-made natural disaster in decades is about to occur.
The area of New Iberia, Louisiana, is dotted with oil wells. Texaco is having a whale of a time poking holes in the ground and seeing what they hit; one of these probing wells is located three hundred yards offshore in 11-foot-deep Lake Peigneur. The presence of salt domes in the area makes it likely that they’ll find pockets of oil beneath the lake, and the presence of the salt mine in the area has made Texaco do some careful calculations so as not to infringe on Diamond Crystal’s territory.
Somebody apparently forgot to carry the three.
On the morning of November 21, the men on the exploratory rig in Lake Peigneur were happily drilling away in the hopes of striking it rich. Over a thousand feet below the surface, the drill bit was chewing its way through rock when it hit something with a considerably different texture and seized up; as the men tried to free it, wondering what was going on, the rig itself suddenly tilted alarmingly toward the water, and they heard some strange and ominous popping sounds.
Wisely, the operators cut loose their barges and got the hell out of it, and watched from the shore as their whole rig continued to tilt and collapse beneath the surface. They knew the lake was only about eleven feet deep, so the disappearance of five million dollars’ worth of equipment was impossible.
So was the fact that a massive whirlpool developed over their drill site.
In the Diamond Crystal mine, something like 1,230 feet below the surface, water was roaring down the Texaco drillshaft into a mine gallery through a hole fourteen inches wide--a hole which rapidly became much larger as the blasting stream of water dissolved the salt. I don’t know the calculations to work out exactly how forceful the initial jet of water would have been, given the width of the drillshaft, the diameter of the opening, and the distance from the surface, but I think it can be safely assumed to be intense.
An electrician in the mine was the first to see the flood approaching, and sounded the alarm: incredibly, all of the miners managed to escape as the water dissolved away supports and collapsed shafts, swirled and frothed and roared in the darkness of the tunnels, driving air before it with such force as to blow the heads off the mineshafts and then send geysers shooting four hundred feet into the air. Excellent emergency planning and mine-evacuation drills were credited with the survival of the miners. Others attribute it to divine providence.
On the surface, onlookers watched in fascinated horror at the demonstration of what happens when you pull the plug at the bottom of a lake. By now the whirlpool was massive, a quarter-mile across, powerful enough to reverse the Delcambre Canal leading to the Gulf of Mexico and suck eleven barges helplessly down into the drowned caverns of the mine. Another drilling platform, quite a lot of an island, and a nearby parking lot vanished as well. As the lake drained away (with what must have been the loudest sucking sound ever heard) the water from the canal poured 164 feet into the lakebed, creating the tallest waterfall in Louisiana.
As children, most people have watched bathwater swirl away down the plughole and wondered on some level whether it would suck them down too; what child hasn’t anxiously asked its parent what would happen if someone pulled the plug on the ocean? I don’t envy the children who were around to watch Lake Peigneur go down the drain. If that can happen, what else have the grownups lied about?
The lake water took about three hours to drain into the mine. After that, water from the Gulf of Mexico via the Delcambre Canal continued to flow into the crater that had been the lakebed, filling up vast and unknown caverns under the earth, replacing freshwater with salt, moving silently through the holes where men had dug and joked and cursed. It took two days before the water level finally rose to the point where the pressure equalized and the suction eased off: nine of the eleven sunken barges resurfaced, leaving the tug and the Texaco rig somewhere in the flooded mine workings.
There are no obvious reports to be found on the internets about investigation into the accident, and–-hilariously–-no official responsibility could be taken, as there was no longer any actual evidence of the Texaco drill shaft breaking through into the salt mine. Texaco paid Diamond Crystal and a neighboring business several million in out-of-court settlements anyway, but the disaster itself erased the evidence required to legally convict its perpetrators.
I have to wonder who was responsible for the miscalculation that sent the drill bit into the mine. I have to wonder what he or she thought when the lake started to go down the drain. This is not just “d’oh,” this is “d’oh” on a scale that changes ecosystems.
Remember, boys and girls, double-checking one’s sums can save a lot of hassle. Next time you’re deciding between pink, black, brown, smoked, kosher, or grey salt to put on your purple Chinese space potato fries, remember how lucky you are not to have to rely on boring old mined rock salt, and the hazards associated with salt mining.
(It’s okay to laugh at Lake Peigneur. It’s a little difficult not to.)
Information for this post was taken from Wiki (yes, I know) and the excellent Damn Interesting article on it. Unfortunately I can't get my hands on any official reports.
Before there was saltnews.com, you got your salt from industrial salt mines. Rock salt, or halite, the stuff that rots the undercarriage of your car in winter, represents ancient salt deposited in marine basins as water evapourated. Over time, the salt beds were covered with layers of sediment and compressed. Salt is less dense than the surrounding rock, and it has a tendency to push upward in blobby formations called salt domes (topographical modeling of these formations looks a lot like the bottom of a lava lamp as it warms up). These domes can be absolutely massive, shouldering aside mountains as they bubble to the surface.
As the salt domes squash and displace strata around and above them, pockets are formed between salt and rock where oil and natural gas can collect. Salt mining operations, therefore, are often found right next to oil/gas drilling operations–including under the Gulf Coast. Mostly this does not present a problem. Mostly.
Imagine a salt mine that is busily chipping away at a salt dome that happens to be directly under a shallow lake. The miners know perfectly well where they can and cannot dig; the tunnels extend far below the lake itself, and the mine is producing a healthy crop of salt for the Diamond Crystal Salt Company. It’s November 21, 1980, and the most bizarre man-made natural disaster in decades is about to occur.
The area of New Iberia, Louisiana, is dotted with oil wells. Texaco is having a whale of a time poking holes in the ground and seeing what they hit; one of these probing wells is located three hundred yards offshore in 11-foot-deep Lake Peigneur. The presence of salt domes in the area makes it likely that they’ll find pockets of oil beneath the lake, and the presence of the salt mine in the area has made Texaco do some careful calculations so as not to infringe on Diamond Crystal’s territory.
Somebody apparently forgot to carry the three.
On the morning of November 21, the men on the exploratory rig in Lake Peigneur were happily drilling away in the hopes of striking it rich. Over a thousand feet below the surface, the drill bit was chewing its way through rock when it hit something with a considerably different texture and seized up; as the men tried to free it, wondering what was going on, the rig itself suddenly tilted alarmingly toward the water, and they heard some strange and ominous popping sounds.
Wisely, the operators cut loose their barges and got the hell out of it, and watched from the shore as their whole rig continued to tilt and collapse beneath the surface. They knew the lake was only about eleven feet deep, so the disappearance of five million dollars’ worth of equipment was impossible.
So was the fact that a massive whirlpool developed over their drill site.
In the Diamond Crystal mine, something like 1,230 feet below the surface, water was roaring down the Texaco drillshaft into a mine gallery through a hole fourteen inches wide--a hole which rapidly became much larger as the blasting stream of water dissolved the salt. I don’t know the calculations to work out exactly how forceful the initial jet of water would have been, given the width of the drillshaft, the diameter of the opening, and the distance from the surface, but I think it can be safely assumed to be intense.
An electrician in the mine was the first to see the flood approaching, and sounded the alarm: incredibly, all of the miners managed to escape as the water dissolved away supports and collapsed shafts, swirled and frothed and roared in the darkness of the tunnels, driving air before it with such force as to blow the heads off the mineshafts and then send geysers shooting four hundred feet into the air. Excellent emergency planning and mine-evacuation drills were credited with the survival of the miners. Others attribute it to divine providence.
On the surface, onlookers watched in fascinated horror at the demonstration of what happens when you pull the plug at the bottom of a lake. By now the whirlpool was massive, a quarter-mile across, powerful enough to reverse the Delcambre Canal leading to the Gulf of Mexico and suck eleven barges helplessly down into the drowned caverns of the mine. Another drilling platform, quite a lot of an island, and a nearby parking lot vanished as well. As the lake drained away (with what must have been the loudest sucking sound ever heard) the water from the canal poured 164 feet into the lakebed, creating the tallest waterfall in Louisiana.
As children, most people have watched bathwater swirl away down the plughole and wondered on some level whether it would suck them down too; what child hasn’t anxiously asked its parent what would happen if someone pulled the plug on the ocean? I don’t envy the children who were around to watch Lake Peigneur go down the drain. If that can happen, what else have the grownups lied about?
The lake water took about three hours to drain into the mine. After that, water from the Gulf of Mexico via the Delcambre Canal continued to flow into the crater that had been the lakebed, filling up vast and unknown caverns under the earth, replacing freshwater with salt, moving silently through the holes where men had dug and joked and cursed. It took two days before the water level finally rose to the point where the pressure equalized and the suction eased off: nine of the eleven sunken barges resurfaced, leaving the tug and the Texaco rig somewhere in the flooded mine workings.
There are no obvious reports to be found on the internets about investigation into the accident, and–-hilariously–-no official responsibility could be taken, as there was no longer any actual evidence of the Texaco drill shaft breaking through into the salt mine. Texaco paid Diamond Crystal and a neighboring business several million in out-of-court settlements anyway, but the disaster itself erased the evidence required to legally convict its perpetrators.
I have to wonder who was responsible for the miscalculation that sent the drill bit into the mine. I have to wonder what he or she thought when the lake started to go down the drain. This is not just “d’oh,” this is “d’oh” on a scale that changes ecosystems.
Remember, boys and girls, double-checking one’s sums can save a lot of hassle. Next time you’re deciding between pink, black, brown, smoked, kosher, or grey salt to put on your purple Chinese space potato fries, remember how lucky you are not to have to rely on boring old mined rock salt, and the hazards associated with salt mining.
(It’s okay to laugh at Lake Peigneur. It’s a little difficult not to.)
Information for this post was taken from Wiki (yes, I know) and the excellent Damn Interesting article on it. Unfortunately I can't get my hands on any official reports.
Monday, June 8, 2009
What went right: how sirens work
Living as I do in the outskirts of Baltimore’s thriving crack district, I hear a lot of sirens. In fact I am rather inured to the sound of sirens after four years of
WHOOOOOOooooooooooOOOOOOOOOOOOoooooooooooOOOOOOOOOO BRAAAAAAAAAA BRAAAAAAAAAA WEEEEEOOOoooooooOOOOOOooooo
but I always sort of wondered what actually made that noise, and how, and if it was really the same as the air-raid sirens you hear in old movies. I don’t know if any of you have looked into the world of sirens, but there’s a corollary to the law of if-it-exists-there-is-porn-of-it: if it exists, there is a small and deranged cadre of people who collect it for purely nonsexual reasons. Good examples of this include vacuum tubes, power-line insulators, and the whole spectrum of the siren family from horns and whistles all the way up to the most ridiculous noisemaker of them all, about which more later.
There are two sorts of siren, for most purposes, and the fire trucks that go under my window multiple times per evening (WHOOOOoooooooooooooOOOOOOOO BRAAAAAAAAAA BRAAAAAA) are equipped with the pneumatic type, plus an air horn, while the police cars (NNEEEEEEEEEEEEEEEEEEEEEEEEEEEeeeeeeeeeeeeEEEEEEEEEEEEEEEEEEEEeeeeeeeeeeeeEEEEEEEEEEE WOOP WOOP EEEEEEEEEEEE) have electronic sirens. The electronic ones can replicate the wail of a pneumatic siren but have a much tinnier sort of noise, higher and more nasal than their mechanical cousins.
Pneumatic sirens work on a principle so simple it’s funny. Sound is perceived as the result of air pressure variations hitting our little tiny delicate eardrums and billowing them in and out, so anything that causes a regular disturbance in airflow will make noise, viz. blowing raspberries. That is in effect what happens when you spin up a pneumatic siren. An impeller fan (rotor) turns inside a slotted housing (stator), sucking air in and blowing it out again through the slots in the stator drum. As the rotor turns, it chops the air-stream coming out of the stator slots into regular bursts. Each time the rotor and stator holes align, a burst of air is forced through. The frequency of these bursts is the pitch of the siren. The alternating pressure wave propagates through the air and drives everybody nuts unless they’ve lived on Lombard Street and have learnt to ignore sirens for the most part.
These are the sirens you will be familiar with from the war films, the mournful minor-third wail of the British Carter air-raid siren and the single tone of the US Federal Thunderbolt. They take a lot of power to spin up to their maximum RPM/pitch, but can do this quickly; there’s no brake on the shaft, so once power is cut off it takes a long time for the siren to spin down out of audio frequency. You’ll notice this next time you hear a fire-truck or a volunteer-firehouse siren spin down: it sounds thoroughly desolate and discouraged. WOOOOOOOOOOooooooooooooooooooooooooooooooooooooooooooooo.
Both the Carter and the Federal are dwarfed by the apotheosis of all sirens, the ridiculous, majestic, and rather scary Chrysler Air Raid Siren. VictorySiren.com has a lot more information about this behemoth, but I shall outline a few of the more salient details for you, because it is just absolutely unbelievable:
This siren is powered by a 180-hp V8 hemi from Chrysler’s industrial engine line. It runs a compressor capable of pushing 2610 cubic feet of air a minute through a rotor spinning at a maximum of 4600 rpm and forcing it out of its six aluminum throats at four hundred miles an hour. Under optimum conditions it can be heard more than thirty miles away. At one hundred feet from the monster its output is 138 dB. It is the loudest sound signaling device ever built. It is also the size of a car and weighs over five thousand pounds.
Looking at the Chrysler siren and listening to clips of it being run is looking into another era. I can’t think of another object that exemplifies the American approach to the Cold War: it’s huge, massively powerful, well-designed, and completely paranoid.
And I want one.
Image credits: airraidsirens.com & Anthony Pollard on airraidsirens.com
WHOOOOOOooooooooooOOOOOOOOOOOOoooooooooooOOOOOOOOOO BRAAAAAAAAAA BRAAAAAAAAAA WEEEEEOOOoooooooOOOOOOooooo
but I always sort of wondered what actually made that noise, and how, and if it was really the same as the air-raid sirens you hear in old movies. I don’t know if any of you have looked into the world of sirens, but there’s a corollary to the law of if-it-exists-there-is-porn-of-it: if it exists, there is a small and deranged cadre of people who collect it for purely nonsexual reasons. Good examples of this include vacuum tubes, power-line insulators, and the whole spectrum of the siren family from horns and whistles all the way up to the most ridiculous noisemaker of them all, about which more later.
There are two sorts of siren, for most purposes, and the fire trucks that go under my window multiple times per evening (WHOOOOoooooooooooooOOOOOOOO BRAAAAAAAAAA BRAAAAAA) are equipped with the pneumatic type, plus an air horn, while the police cars (NNEEEEEEEEEEEEEEEEEEEEEEEEEEEeeeeeeeeeeeeEEEEEEEEEEEEEEEEEEEEeeeeeeeeeeeeEEEEEEEEEEE WOOP WOOP EEEEEEEEEEEE) have electronic sirens. The electronic ones can replicate the wail of a pneumatic siren but have a much tinnier sort of noise, higher and more nasal than their mechanical cousins.
Pneumatic sirens work on a principle so simple it’s funny. Sound is perceived as the result of air pressure variations hitting our little tiny delicate eardrums and billowing them in and out, so anything that causes a regular disturbance in airflow will make noise, viz. blowing raspberries. That is in effect what happens when you spin up a pneumatic siren. An impeller fan (rotor) turns inside a slotted housing (stator), sucking air in and blowing it out again through the slots in the stator drum. As the rotor turns, it chops the air-stream coming out of the stator slots into regular bursts. Each time the rotor and stator holes align, a burst of air is forced through. The frequency of these bursts is the pitch of the siren. The alternating pressure wave propagates through the air and drives everybody nuts unless they’ve lived on Lombard Street and have learnt to ignore sirens for the most part.
These are the sirens you will be familiar with from the war films, the mournful minor-third wail of the British Carter air-raid siren and the single tone of the US Federal Thunderbolt. They take a lot of power to spin up to their maximum RPM/pitch, but can do this quickly; there’s no brake on the shaft, so once power is cut off it takes a long time for the siren to spin down out of audio frequency. You’ll notice this next time you hear a fire-truck or a volunteer-firehouse siren spin down: it sounds thoroughly desolate and discouraged. WOOOOOOOOOOooooooooooooooooooooooooooooooooooooooooooooo.
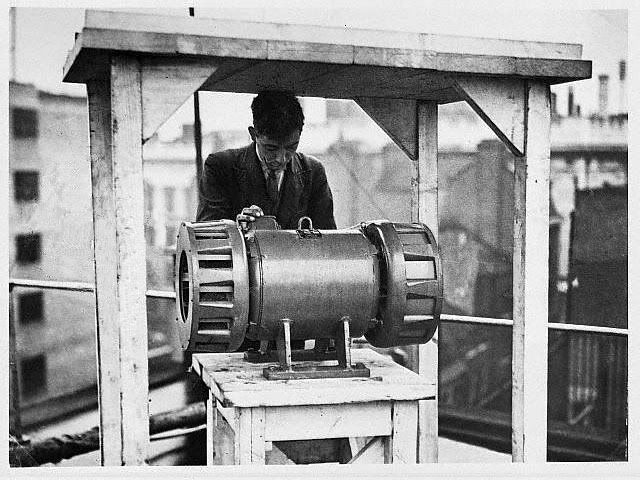{kind=link}
{kind=link}
Both the Carter and the Federal are dwarfed by the apotheosis of all sirens, the ridiculous, majestic, and rather scary Chrysler Air Raid Siren. VictorySiren.com has a lot more information about this behemoth, but I shall outline a few of the more salient details for you, because it is just absolutely unbelievable:
This siren is powered by a 180-hp V8 hemi from Chrysler’s industrial engine line. It runs a compressor capable of pushing 2610 cubic feet of air a minute through a rotor spinning at a maximum of 4600 rpm and forcing it out of its six aluminum throats at four hundred miles an hour. Under optimum conditions it can be heard more than thirty miles away. At one hundred feet from the monster its output is 138 dB. It is the loudest sound signaling device ever built. It is also the size of a car and weighs over five thousand pounds.
Looking at the Chrysler siren and listening to clips of it being run is looking into another era. I can’t think of another object that exemplifies the American approach to the Cold War: it’s huge, massively powerful, well-designed, and completely paranoid.
And I want one.
Image credits: airraidsirens.com & Anthony Pollard on airraidsirens.com
Friday, June 5, 2009
Death in a cloud: the Bhopal disaster
Even a brief foray into researching the causes, immediate consequences, and long-term repercussions of the gas disaster at Bhopal in 1984 quickly demonstrates that in order to cover all the aspects of the event fully one would need to write a book, not a blog post. Since other people with access to primary sources have already done this for me, and I refer here to Ingrid Eckerman's fantastic The Bhopal Saga, I will try to avoid doing so, although this is going to be long.
Bhopal is the capital of the Indian state of Madhya Pradesh, located more or less in the middle of the country. It's the second-biggest city in the state, and is--or was--known as the City of Lakes for the multiple natural and man-made lakes in and around the city itself. Union Carbide India Limited (UCIL) had built a chemical manufacturing plant in East Bhopal City in 1969, the same year the ValuJet DC-9 plane was built, which was owned partly by Union Carbide Corporation (UCC) and partly by Indian authorities, although Union Carbide owned all the designs and processes used at the site.
UCIL Bhopal's main product was the insecticide carbaryl. Sold under the trademark Sevin, carbaryl is one of a group of chemicals called carbamates which happen to be cholinesterase inhibitors, meaning that they prevent the enzyme cholinesterase from breaking down the neurotransmitter acetylcholine and therefore do extremely unkind things to the human nervous system; without cholinesterase getting rid of the acetylcholine sitting around in synaptic clefts, the nerves controlling our muscles don't stop firing, causing neuromuscular paralysis and eventual death. So we can see that carbaryl and its relatives aren't necessarily something you want large quantities of in your back yard; however, much like methamphetamine, the process used to make this nasty substance is even more dangerous and poisonous than the substance itself. One particular compound required to make carbaryl at the Bhopal plant is methyl isocyanate, or MIC. MIC killed an unknown number of people, probably between 8,000 and 10,000, in and around Bhopal on the night of December 2-3, 1984--and continues to claim victims today, as survivors of the Bhopal disaster slowly succumb to exposure-related illnesses.
I cannot emphasize enough how absolutely nightmarish the Bhopal plant was--and is to this day--in terms of toxic chemicals. MIC will kill you, but so will chlorine, phosphene, methyl carbamyl chloride, monomethylamine, cyanuric acid, hydrogen chloride, and all the other multisyllabic substances involved in and resulting from the production of carbaryl. Over here in the States when we think of toxic chemicals Woburn and Love Canal and Valley of the Drums and Hinkley come to mind: what happened at Bhopal casts all the chemical accidents in the US far into the shade. Here was not a royal fellowship of death, but a treasure-house of it; an Aladdin's cave of substances inimical to human life and health, all sitting within a hundred yards of the poorest shanties of Bhopal.
In order to make Sevin, you need to combine chlorine and carbon monoxide to form phosgene, then combine that with monomethylamine and chloroform to produce methyl carbamyl chloride (and hydrogen chloride gas). You then break down the methyl carbamyl chloride into methyl isocyanate, which you react with alpha-naphthol and carbon tetrachloride to finally produce carbaryl. There is a separate process by which you can make carbaryl without using MIC, but it costs more, so it wasn't an option.
Now do that on an industrial scale with profit as the priority, with poorly maintained equipment, poorly trained or untrained workers, poorly trained or untrained supervisors ignorant of the physiological effects of the substances they were handling, and set your manufacturing plant within pebble-throwing distance of residential neighborhoods without telling the inhabitants what your process involves or what to do in a chemical-release emergency (other than that you make "medicine" for crops), and you’ve got UCIL’s operation at Bhopal to a T. UCIL did provide Bhopal hospitals with some resuscitation equipment, but provided no emergency procedures for gas-release incidents.
MIC, as a crucial ingredient in the carbaryl manufacturing process, was required in large amounts on the site. When the plant was built, UCIL only manufactured carbamate pesticides from concentrated ingredients shipped in from the US: however, in 1980, UCIL equipped the Bhopal plant with the necessary setup to manufacture it from chlorine (brought in from external suppliers) and carbon monoxide produced on-site. MIC was stored in two of three main tanks, designated 610, 611, and 619; the Union Carbide manual stated that only two of the tanks were to be used for storage at any given time, that the tanks' contents be refrigerated to five degrees centigrade or below and kept under a controlled pressure of nitrogen gas, and that the tanks and fittings should be made out of stainless steel and not any other alloy (including carbon steel).
The tanks were designed with a relief valve vent header (RVVH) which led directly to a vent gas scrubber (VGH) which bubbled the escaping gas through a solution of lye to neutralize it before burning it off from the plant's flare tower or releasing it from the stack. In the event of a tank reaching its pressurization limit (40 pounds per square inch over atmospheric pressure, or psig), a rupture disk would burst, a relief valve would open, and the gas would be released to the vent scrubber. As MIC reacts with water, a nitrogen pressurization system was built in to ensure the dry nitrogen atmosphere inside the tanks wouldn't become contaminated with moisture from the air: if a tank's pressure fell below 2 psig, nitrogen would be pumped into the tank through a connector to a second line running from tank to scrubber, the process vent header (PVH). We have at this point two main routes for gas to escape from any one of the three MIC storage tanks: the RVVH and the PVH.
Piping in the plant was prone to developing clogs due to corrosion or deposited salts from the chemicals running through them, and washing out of the pipes with water was a commonplace task. A barrier, called a slip-bind or slip-blind depending on your source, should have been inserted into the pipes in question to ensure water didn't escape the section being washed out. This very important safety procedure was apparently left out of the written instructions provided to workers for washing out the pipes, according to Eckerman, who cites the Union Research Group of Mumbai (Bombay)'s 1985 report, The role of management practices in the Bhopal gas leak disaster.
In addition to the incomplete procedure instructions, the Bhopal plant lacked a rather damning number of security measures that a similarly purposed US Union Carbide plant considered necessary for operation, contrary to UCC's initial insistence that Bhopal was run to the same standard as its stateside plants. Eckerman offers a table of the security features at UCC's plant in Virginia that were not available/implemented in Bhopal, including:
--Non-MIC carbaryl production process (patented by UCC)
--Storage of MIC only in small quantities, in small vessels, for short times
--Fully-computerized four-stage alarm system
--Monitoring of chemical inventory
--"Knock-down" tank to handle MIC overflows before they could be released
--Emergency VGS with extra capacity
--VGS and flare tower available at all times, not just when MIC was being produced
--Refrigeration with backup refrigeration system to keep MIC at -10 degrees C
--Exclusive stainless steel construction
--Location downwind, outside of town
--Siren/alarm system pointed outward and capable of alerting residents of town
In the initial years of the Bhopal plant's self-sufficient MIC/carbaryl production era, it was run by an American engineer who was committed to safety. In 1982, he was replaced with an Indian engineer educated in the States, directly subordinate to a financial controller most interested in reducing/controlling the company's losses. This is when it started down the garden path to hell, and the first few steps along that path were to screw up staffing/hiring policies for the MIC plant and fire a bunch of employees, as well as cutting down training from 6 months to 8 weeks--which, according to some of the workers, were barely sufficient to give them the necessary skills. When one worker complained about being asked to take on the role of a full-fledged operator after 5 weeks of training, he was apparently allowed to complete the final three.
On the night of the disaster, there were no trained engineers on the site. And this is not making Play-Doh or putting the lids on pies, this is life-and-death stuff they're dealing with.
Eckerman's list of malfunctioning, disconnected, or nonexistent safety systems at Bhopal reads like a disaster movie's build-up stage. Surely no one could have let this go on in real life? Surely all these systems could not be malfunctioning this badly at once? Didn't anyone care?
Probably they did, but it was more than their jobs were worth to complain. The Bhopal plant had been granted a license to produce something like 5,000 tons of pesticide a year. In point of fact they were selling around 2,000. People who knew the Indian market had asked that a smaller plant be built, but this had been bulldozed over by UCC, with the predictable result that Bhopal was run at a loss and the UCIL management was constantly trying to cut costs and raise profits: thus the staffing cuts, thus the replacement of stainless valving and pipes with carbon steel, thus the draining of the MIC refrigeration unit and the use of the system's freon in other plant operations. One after one after one, the systems that should have prevented Bhopal's disaster were deliberately shut down, either to save money or because they just weren't working right.
Unsurprisingly, there had been "warning" accidents in the months leading up to December 84. MIC exposure accidents, leaks of MIC, chlorine, monomethylamine, phosgene, and carbon tetrachloride (sometimes in combination); rather dreadfully, Eckerman mentions that "a journalist...had listened to the workers' discussions about the dangers at the factory--toxic gases, deadly leaks, and the likelihood of explosions. After having done some research, he started to write articles in the local press, warning of the hazards associated with the plant. His final article, which appeared just five months before the disaster, was titled 'Bhopal on the Brink of a Disaster.' No one took any notice. He also sent letters where he summarized the findings of his investigations to the Chief Minister and the Chief Justice of the Supreme Court, and requested them to close down the factory. He got no answer."
Tank 610, which would eventually kill something more than twenty thousand people, was causing problems long before the accident itself. Eckerman writes that on October 21, 1984, less than two months before the disaster, it could not be pressurized; managers switched to tank 611, more biddable, to continue Sevin production. Nobody bothered to find out why 610 misbehaved. On November 30 (or 26, depending on sources) nitro pressure in 611 fell, making them wonder what the hell was wrong with these here tanks in this here plant and causing an investigation that ended with the replacement of a faulty valve on tank 611--and the abandonment of 610. "Operators later told journalists that every time nitrogen was pumped in [to tank 610], it leaked out again through an unknown route."
Let's skip ahead, shall we? Tanks 619, 611 and the recalcitrant 610 are entombed in a concrete mound some distance from the Sevin unit and flare stack. On the night of the accident, the following conditions existed:
1) Tank temperatures were not being logged
2) The vent gas scrubber (VGS) was not in use (this does not entirely fit with some reports of the sodium hydroxide scrubber solution registering a temperature, on the morning after the accident, that indicated a reaction had taken place)
3) The refrigeration system on the MIC tanks was not in use and could not be activated as its refrigerant had been nicked for use elsewhere onsite
4) A slip bind was not used when the pipes were being washed
5) The concentration of chloroform in 610 was too high
6) The tank was not pressurized with nitrogen (or anything else)
7) The tank's high-temp alarm was not functioning
8) The evacuation tank (619) was not empty
There are several major reports covering the incident itself, which most people agree began with water washing of some of the pipelines of the plant. Supervisors on duty at the time were not familiar with the factory's complex maintenance procedures, and knew nothing about MIC or phosgene: in fact the supervisor was convinced that there could not be a leak when production of MIC had been stopped.
The 1988 Arthur D. Little Inc. report, which UCC used to support the sabotage theory, states the following:
"Shortly before the end of the second shift, at 10:20 p.m., the pressure in Tank 610 was reported to be at 2 psig. The shift change occurred at 10:45 p.m., and everything was normal until 11:30 p.m., at which time a small leak was reported downwind and in the area of the MIC production unit. The MIC supervisor said that he would deal with the leak after tea, which began at 12:15 a.m. The tea lasted until 12:40 a.m. at which time all was normal. At that point, the control room operator observed the pressure rise suddenly in Tank 610, and within minutes the indicator was off the gauge's scale. At 12:45 a.m., the safety valve on the tank opened, and gas came out of the stack of the vent gas scrubber. The operators ran to the tank and found it rumbling, and the concrete over the tank was cracking. The fire squad sprayed the stack to knock down the gas, and the reaction subsided an hour or so later. The workers claimed to have no idea as to why the pressure rose in the first instance. According to this account, the incident occurred suddenly and inexplicably."
This is at best disingenuous. Water--a considerable amount of it, thousands of pounds--entered tank 610, and there was evidence of an MIC leak before the main catastrophe that was going to be dealt with "after tea." The boy whose job it was to bring the control room operators their nice tea for their break noted that there was a seriously taut atmosphere and nobody for some reason actually took him up on his tea offer. This was uncharacteristic.
The thing about water and MIC is that they react like eighties movie teenagers and produce a hell of a lot of heat. They produce even more heat in the presence of iron, which would have been present in the contaminant water due to pipe corrosion (carbon steel was used in place of stainless to keep costs down). MIC is such an unstable chemical that it reacts with itself under the right circumstances, and in tank 610, it was gleefully doing so in an exothermic sort of way, creating more heat with every single atom undergoing change, and in a very short time this pressure exceeded the 40 psig tank rupture disk, releasing MIC and a bunch of other chemicals directly to the vent gas scrubber. Which would have meant something, had the VGS a) been working or b) been capable of handling a release of this magnitude.
Times for the various events occurring during the disaster vary. Here's a summary from Eckerman directly off Google Books, which contradicts the timeline Wikipedia presents:
20:30 (8:30 PM): Press in 610 noted as 2 psig. Operator told to wash out lines close to MIC tank(s). Presumably, not provably, operators failed to install slip-binds (due to incomplete instructions) and allowed water to flow freely through the piping of the relief valve vent header and/or the process valve vent header. Various accounts state that operators did not use slip-binds, that they noticed water was not coming out of bleeder lines and shut off the water flow, and that supervisors then ordered them to resume the flow.
22:00 (10:00 PM): Approximate time when water began to enter (presumably unpressurized) tank containing 42 tonnes of MIC minus refrigeration. Reaction begins.
22:30 (10:30 PM): one report states that workers told to use water to continue to clean lines (i.e. keep tap running) and that night shift would turn it off; new operators came on duty, poor bastards, and logged 610's pressure as 2 psi. Alternate reports state that shift change occurred at 10:45 or 11. Some reports mention throat and eye irritation from a MIC leak close to the area where the lines were being washed around 10:45.
23:00 (11:00 PM) One report marks the first report of an MIC leak by a field operator by the VGS; operator said later that the press was 2 psi, but in other reports is mentioned as saying that the 2 psi reading was 3 hours old.
23:30 (11:30 PM) Last transfer of MIC to the Sevin unit. Seems to have come from tank 610 not 611. In addition:
-'The operators on ground level noticed dirty water spilling from a higher level in the MIC structure and MIC in the atmosphere. The MIC and dirty water were coming out of a branch of the RVVH. The pressure safety valve had been removed and the open end of the RVVH branch line was not blinded.'
-'The operators found brownish water and steam coming out from a drain-cock eight yards off the ground. The supervisor recommended turning off the taps after the tea break. The team left for the staff cafeteria.'
The really telling point is 12:15 PM, when the transfer of MIC from tank 611 to the Sevin unit occurred, which UCC investigators concluded to be an attempt by MIC operators to remove water from the tank. We don't know how the water got in there: we just know it did, and while the Arthur D. Little company and UCC continue to maintain it was due to one or more disgruntled operators squirting water into the MIC tank (despite the fact that doing this would most likely kill him or her very horribly) rather than sheer incompetence, there is no conclusive evidence for the sabotage.
All the reports seem to agree that 12:15 is when things started to go very badly wrong. Pressure in tank 610 was rising through 30 psig and off the scale, which pegged at 55; when control room operators and supervisors ran to have a look at it, they found the tank moving, rumbling, cracking the concrete over it with its vibration and heat expansion, and so hot as to flash cooling water off into steam. One report states that the tank stood on end and fell back again, but did not burst. They ran like hell back to the control room and turned on the VGS system, but couldn't verify that it was working.
It was now 12:30, and clouds of lethal gas were spewing from the plant stack and spreading rapidly through Bhopal. Accounts differ on when the siren was sounded, anywhere from 12:15 to 1 AM, but it was shut off shortly thereafter. Attempts were made to knock down the gas release by spraying water at it, but the sprays couldn't reach high enough to make a difference. One worker was killed when he tried to climb the stack assembly and somehow shut off the release; he was almost immediately overcome by the gas and fell off, breaking several bones. By 1:30, workers were running for their lives: people who lived close to the plant were already dying.
Tank 610 continued to pour MIC and a host of other toxins into the night air until it was empty; some reports mention that the safety valve reclosed (as the pressure fell below 40 psig) around 2:30, and the emission stopped. By now 42 tonnes of deadly gas were flowing through Bhopal, blinding and choking people in their beds.
MIC is heavier than air; it hugs the ground, rolling downhill. The weather conditions on the night of the accident were as bad as they could be: a temperature inversion trapped the gases close to the ground, and there wasn't enough wind to blow the cloud away. There's been considerable controversy over the role played by hydrogen cyanide (HCN) in the deaths at Bhopal: MIC breaks down into HCN at high temperatures, and tank 610 may have reached sufficient temperatures to allow this reaction. Cyanide was found in the bodies of some Bhopal victims, and scientists have merrily argued about which of the many gases making up the lethal cloud was responsible for the deaths, which strikes me as missing the point.
The people of Bhopal were awakened by acute pain in their eyes, noses, and throats; coughing uncontrollably, blinded by tears, vomiting, they fled into the streets to escape. People were trampled to death in the rush to evacuate. Mothers lost their babies when they were literally pulled from their arms by the force of people struggling to push through the crowd. Because MIC is so heavy, concentrations of it were worst right over the ground; the shortest people--children--got the heaviest doses. Many of those who did not die at once succumbed at the grossly unprepared hospitals, drowning as pulmonary edema filled their lungs with fluid or suffocating as their devastated bronchi went into intractable spasm. Doctors had no idea what was responsible for the injuries; eye drops and cough medicine were handed out and glucose drips set up. Bodies were everywhere, piled on one another, littering the streets.
Dawn brought with it evidence of the extent of the disaster. Thousands of bodies--of livestock as well as people--lay where they had fallen. Within a few days every tree in Bhopal lost its leaves, and the grass turned yellow: a blight of biblical proportions. Police trucks carried bodies to be dumped in the river; others were stacked into funeral pyres. Official procedure for identifying the dead was left behind in the rush to clear the city of the dead; we don't know how many people died that night, but initial reports listed the death toll at over two thousand. That figure jumped to 8,000 and then to 10,000 as more and more died of their injuries. All in all, UCIL killed more than twenty thousand people with one accident.
In the wake of the disaster, UCC was faced not only with attempting to address the devastating leak that had occurred, but with preventing another leak. Tonnes of MIC still remained in the other holding tanks, and it was determined that the thing to do was to convert this into Sevin as soon as possible. "Operation Faith" was conducted on December 16, but this time rigorous safety measures were in place and the inhabitants--remaining inhabitants--of Bhopal were evacuated prior to the procedure. Bhopal residents had absolutely no trust left for the authorities; everyone who could fled the city with all their belongings.
It is beyond the scope of this write-up to cover the reaction to Bhopal, or the years which followed. Suffice it to say that this must not be forgotten, that the rest of the world must know about it, tell the next generation what happened. Those who died at Bhopal mattered, and the grossly negligent maintenance and staffing of the UCIL plant that killed them also matters. Remembering Bhopal is remembering that accidents like this can happen, and that the corporations responsible for accidents must make preventing such accidents their priority; that profit does not trump human lives, and that decisions made in a boardroom affect the everyday existence of hundreds of thousands on the other side of the world.
And that's what went wrong.
Information in this post was taken from the following sources:
Eckerman, Ingrid (2004). The Bhopal Saga — Causes and Consequences of the World's Largest Industrial Disaster. India: Universities Press. ISBN 81-7371-515-7. Available via Google Books.
Kalelkar AS, Little AD. (1998) Investigation of Large-magnitude incidents: Bhopal as a Case Study..PDF available. London: The Institution of Chemical Engineers Conference on Preventing Major Chemical Accidents (Arthur D. Little Report)
Labunska I, Stephenson A, Brigden K, Stringer R, Santillo D, Johnston P.A. (1999). The Bhopal Legacy. Toxic contaminants at the former Union Carbide factory site,Bhopal, India: 15 years after the Bhopal accident. PDF available. Greenpeace Research Laboratories, Department of Biological Sciences, University of Exeter, Exeter UK
Stringer R, Labunska I, Brigden K, Santillo D. (2002). "Chemical Stockpiles at Union Carbide India Limited in Bhopal: An investigation". Greenpeace Research Laboratories. PDF available.
Bhopal is the capital of the Indian state of Madhya Pradesh, located more or less in the middle of the country. It's the second-biggest city in the state, and is--or was--known as the City of Lakes for the multiple natural and man-made lakes in and around the city itself. Union Carbide India Limited (UCIL) had built a chemical manufacturing plant in East Bhopal City in 1969, the same year the ValuJet DC-9 plane was built, which was owned partly by Union Carbide Corporation (UCC) and partly by Indian authorities, although Union Carbide owned all the designs and processes used at the site.
UCIL Bhopal's main product was the insecticide carbaryl. Sold under the trademark Sevin, carbaryl is one of a group of chemicals called carbamates which happen to be cholinesterase inhibitors, meaning that they prevent the enzyme cholinesterase from breaking down the neurotransmitter acetylcholine and therefore do extremely unkind things to the human nervous system; without cholinesterase getting rid of the acetylcholine sitting around in synaptic clefts, the nerves controlling our muscles don't stop firing, causing neuromuscular paralysis and eventual death. So we can see that carbaryl and its relatives aren't necessarily something you want large quantities of in your back yard; however, much like methamphetamine, the process used to make this nasty substance is even more dangerous and poisonous than the substance itself. One particular compound required to make carbaryl at the Bhopal plant is methyl isocyanate, or MIC. MIC killed an unknown number of people, probably between 8,000 and 10,000, in and around Bhopal on the night of December 2-3, 1984--and continues to claim victims today, as survivors of the Bhopal disaster slowly succumb to exposure-related illnesses.
I cannot emphasize enough how absolutely nightmarish the Bhopal plant was--and is to this day--in terms of toxic chemicals. MIC will kill you, but so will chlorine, phosphene, methyl carbamyl chloride, monomethylamine, cyanuric acid, hydrogen chloride, and all the other multisyllabic substances involved in and resulting from the production of carbaryl. Over here in the States when we think of toxic chemicals Woburn and Love Canal and Valley of the Drums and Hinkley come to mind: what happened at Bhopal casts all the chemical accidents in the US far into the shade. Here was not a royal fellowship of death, but a treasure-house of it; an Aladdin's cave of substances inimical to human life and health, all sitting within a hundred yards of the poorest shanties of Bhopal.
In order to make Sevin, you need to combine chlorine and carbon monoxide to form phosgene, then combine that with monomethylamine and chloroform to produce methyl carbamyl chloride (and hydrogen chloride gas). You then break down the methyl carbamyl chloride into methyl isocyanate, which you react with alpha-naphthol and carbon tetrachloride to finally produce carbaryl. There is a separate process by which you can make carbaryl without using MIC, but it costs more, so it wasn't an option.
Now do that on an industrial scale with profit as the priority, with poorly maintained equipment, poorly trained or untrained workers, poorly trained or untrained supervisors ignorant of the physiological effects of the substances they were handling, and set your manufacturing plant within pebble-throwing distance of residential neighborhoods without telling the inhabitants what your process involves or what to do in a chemical-release emergency (other than that you make "medicine" for crops), and you’ve got UCIL’s operation at Bhopal to a T. UCIL did provide Bhopal hospitals with some resuscitation equipment, but provided no emergency procedures for gas-release incidents.
MIC, as a crucial ingredient in the carbaryl manufacturing process, was required in large amounts on the site. When the plant was built, UCIL only manufactured carbamate pesticides from concentrated ingredients shipped in from the US: however, in 1980, UCIL equipped the Bhopal plant with the necessary setup to manufacture it from chlorine (brought in from external suppliers) and carbon monoxide produced on-site. MIC was stored in two of three main tanks, designated 610, 611, and 619; the Union Carbide manual stated that only two of the tanks were to be used for storage at any given time, that the tanks' contents be refrigerated to five degrees centigrade or below and kept under a controlled pressure of nitrogen gas, and that the tanks and fittings should be made out of stainless steel and not any other alloy (including carbon steel).
The tanks were designed with a relief valve vent header (RVVH) which led directly to a vent gas scrubber (VGH) which bubbled the escaping gas through a solution of lye to neutralize it before burning it off from the plant's flare tower or releasing it from the stack. In the event of a tank reaching its pressurization limit (40 pounds per square inch over atmospheric pressure, or psig), a rupture disk would burst, a relief valve would open, and the gas would be released to the vent scrubber. As MIC reacts with water, a nitrogen pressurization system was built in to ensure the dry nitrogen atmosphere inside the tanks wouldn't become contaminated with moisture from the air: if a tank's pressure fell below 2 psig, nitrogen would be pumped into the tank through a connector to a second line running from tank to scrubber, the process vent header (PVH). We have at this point two main routes for gas to escape from any one of the three MIC storage tanks: the RVVH and the PVH.
Piping in the plant was prone to developing clogs due to corrosion or deposited salts from the chemicals running through them, and washing out of the pipes with water was a commonplace task. A barrier, called a slip-bind or slip-blind depending on your source, should have been inserted into the pipes in question to ensure water didn't escape the section being washed out. This very important safety procedure was apparently left out of the written instructions provided to workers for washing out the pipes, according to Eckerman, who cites the Union Research Group of Mumbai (Bombay)'s 1985 report, The role of management practices in the Bhopal gas leak disaster.
In addition to the incomplete procedure instructions, the Bhopal plant lacked a rather damning number of security measures that a similarly purposed US Union Carbide plant considered necessary for operation, contrary to UCC's initial insistence that Bhopal was run to the same standard as its stateside plants. Eckerman offers a table of the security features at UCC's plant in Virginia that were not available/implemented in Bhopal, including:
--Non-MIC carbaryl production process (patented by UCC)
--Storage of MIC only in small quantities, in small vessels, for short times
--Fully-computerized four-stage alarm system
--Monitoring of chemical inventory
--"Knock-down" tank to handle MIC overflows before they could be released
--Emergency VGS with extra capacity
--VGS and flare tower available at all times, not just when MIC was being produced
--Refrigeration with backup refrigeration system to keep MIC at -10 degrees C
--Exclusive stainless steel construction
--Location downwind, outside of town
--Siren/alarm system pointed outward and capable of alerting residents of town
In the initial years of the Bhopal plant's self-sufficient MIC/carbaryl production era, it was run by an American engineer who was committed to safety. In 1982, he was replaced with an Indian engineer educated in the States, directly subordinate to a financial controller most interested in reducing/controlling the company's losses. This is when it started down the garden path to hell, and the first few steps along that path were to screw up staffing/hiring policies for the MIC plant and fire a bunch of employees, as well as cutting down training from 6 months to 8 weeks--which, according to some of the workers, were barely sufficient to give them the necessary skills. When one worker complained about being asked to take on the role of a full-fledged operator after 5 weeks of training, he was apparently allowed to complete the final three.
On the night of the disaster, there were no trained engineers on the site. And this is not making Play-Doh or putting the lids on pies, this is life-and-death stuff they're dealing with.
Eckerman's list of malfunctioning, disconnected, or nonexistent safety systems at Bhopal reads like a disaster movie's build-up stage. Surely no one could have let this go on in real life? Surely all these systems could not be malfunctioning this badly at once? Didn't anyone care?
Probably they did, but it was more than their jobs were worth to complain. The Bhopal plant had been granted a license to produce something like 5,000 tons of pesticide a year. In point of fact they were selling around 2,000. People who knew the Indian market had asked that a smaller plant be built, but this had been bulldozed over by UCC, with the predictable result that Bhopal was run at a loss and the UCIL management was constantly trying to cut costs and raise profits: thus the staffing cuts, thus the replacement of stainless valving and pipes with carbon steel, thus the draining of the MIC refrigeration unit and the use of the system's freon in other plant operations. One after one after one, the systems that should have prevented Bhopal's disaster were deliberately shut down, either to save money or because they just weren't working right.
Unsurprisingly, there had been "warning" accidents in the months leading up to December 84. MIC exposure accidents, leaks of MIC, chlorine, monomethylamine, phosgene, and carbon tetrachloride (sometimes in combination); rather dreadfully, Eckerman mentions that "a journalist...had listened to the workers' discussions about the dangers at the factory--toxic gases, deadly leaks, and the likelihood of explosions. After having done some research, he started to write articles in the local press, warning of the hazards associated with the plant. His final article, which appeared just five months before the disaster, was titled 'Bhopal on the Brink of a Disaster.' No one took any notice. He also sent letters where he summarized the findings of his investigations to the Chief Minister and the Chief Justice of the Supreme Court, and requested them to close down the factory. He got no answer."
Tank 610, which would eventually kill something more than twenty thousand people, was causing problems long before the accident itself. Eckerman writes that on October 21, 1984, less than two months before the disaster, it could not be pressurized; managers switched to tank 611, more biddable, to continue Sevin production. Nobody bothered to find out why 610 misbehaved. On November 30 (or 26, depending on sources) nitro pressure in 611 fell, making them wonder what the hell was wrong with these here tanks in this here plant and causing an investigation that ended with the replacement of a faulty valve on tank 611--and the abandonment of 610. "Operators later told journalists that every time nitrogen was pumped in [to tank 610], it leaked out again through an unknown route."
Let's skip ahead, shall we? Tanks 619, 611 and the recalcitrant 610 are entombed in a concrete mound some distance from the Sevin unit and flare stack. On the night of the accident, the following conditions existed:
1) Tank temperatures were not being logged
2) The vent gas scrubber (VGS) was not in use (this does not entirely fit with some reports of the sodium hydroxide scrubber solution registering a temperature, on the morning after the accident, that indicated a reaction had taken place)
3) The refrigeration system on the MIC tanks was not in use and could not be activated as its refrigerant had been nicked for use elsewhere onsite
4) A slip bind was not used when the pipes were being washed
5) The concentration of chloroform in 610 was too high
6) The tank was not pressurized with nitrogen (or anything else)
7) The tank's high-temp alarm was not functioning
8) The evacuation tank (619) was not empty
There are several major reports covering the incident itself, which most people agree began with water washing of some of the pipelines of the plant. Supervisors on duty at the time were not familiar with the factory's complex maintenance procedures, and knew nothing about MIC or phosgene: in fact the supervisor was convinced that there could not be a leak when production of MIC had been stopped.
The 1988 Arthur D. Little Inc. report, which UCC used to support the sabotage theory, states the following:
"Shortly before the end of the second shift, at 10:20 p.m., the pressure in Tank 610 was reported to be at 2 psig. The shift change occurred at 10:45 p.m., and everything was normal until 11:30 p.m., at which time a small leak was reported downwind and in the area of the MIC production unit. The MIC supervisor said that he would deal with the leak after tea, which began at 12:15 a.m. The tea lasted until 12:40 a.m. at which time all was normal. At that point, the control room operator observed the pressure rise suddenly in Tank 610, and within minutes the indicator was off the gauge's scale. At 12:45 a.m., the safety valve on the tank opened, and gas came out of the stack of the vent gas scrubber. The operators ran to the tank and found it rumbling, and the concrete over the tank was cracking. The fire squad sprayed the stack to knock down the gas, and the reaction subsided an hour or so later. The workers claimed to have no idea as to why the pressure rose in the first instance. According to this account, the incident occurred suddenly and inexplicably."
This is at best disingenuous. Water--a considerable amount of it, thousands of pounds--entered tank 610, and there was evidence of an MIC leak before the main catastrophe that was going to be dealt with "after tea." The boy whose job it was to bring the control room operators their nice tea for their break noted that there was a seriously taut atmosphere and nobody for some reason actually took him up on his tea offer. This was uncharacteristic.
The thing about water and MIC is that they react like eighties movie teenagers and produce a hell of a lot of heat. They produce even more heat in the presence of iron, which would have been present in the contaminant water due to pipe corrosion (carbon steel was used in place of stainless to keep costs down). MIC is such an unstable chemical that it reacts with itself under the right circumstances, and in tank 610, it was gleefully doing so in an exothermic sort of way, creating more heat with every single atom undergoing change, and in a very short time this pressure exceeded the 40 psig tank rupture disk, releasing MIC and a bunch of other chemicals directly to the vent gas scrubber. Which would have meant something, had the VGS a) been working or b) been capable of handling a release of this magnitude.
Times for the various events occurring during the disaster vary. Here's a summary from Eckerman directly off Google Books, which contradicts the timeline Wikipedia presents:
20:30 (8:30 PM): Press in 610 noted as 2 psig. Operator told to wash out lines close to MIC tank(s). Presumably, not provably, operators failed to install slip-binds (due to incomplete instructions) and allowed water to flow freely through the piping of the relief valve vent header and/or the process valve vent header. Various accounts state that operators did not use slip-binds, that they noticed water was not coming out of bleeder lines and shut off the water flow, and that supervisors then ordered them to resume the flow.
22:00 (10:00 PM): Approximate time when water began to enter (presumably unpressurized) tank containing 42 tonnes of MIC minus refrigeration. Reaction begins.
22:30 (10:30 PM): one report states that workers told to use water to continue to clean lines (i.e. keep tap running) and that night shift would turn it off; new operators came on duty, poor bastards, and logged 610's pressure as 2 psi. Alternate reports state that shift change occurred at 10:45 or 11. Some reports mention throat and eye irritation from a MIC leak close to the area where the lines were being washed around 10:45.
23:00 (11:00 PM) One report marks the first report of an MIC leak by a field operator by the VGS; operator said later that the press was 2 psi, but in other reports is mentioned as saying that the 2 psi reading was 3 hours old.
23:30 (11:30 PM) Last transfer of MIC to the Sevin unit. Seems to have come from tank 610 not 611. In addition:
-'The operators on ground level noticed dirty water spilling from a higher level in the MIC structure and MIC in the atmosphere. The MIC and dirty water were coming out of a branch of the RVVH. The pressure safety valve had been removed and the open end of the RVVH branch line was not blinded.'
-'The operators found brownish water and steam coming out from a drain-cock eight yards off the ground. The supervisor recommended turning off the taps after the tea break. The team left for the staff cafeteria.'
The really telling point is 12:15 PM, when the transfer of MIC from tank 611 to the Sevin unit occurred, which UCC investigators concluded to be an attempt by MIC operators to remove water from the tank. We don't know how the water got in there: we just know it did, and while the Arthur D. Little company and UCC continue to maintain it was due to one or more disgruntled operators squirting water into the MIC tank (despite the fact that doing this would most likely kill him or her very horribly) rather than sheer incompetence, there is no conclusive evidence for the sabotage.
All the reports seem to agree that 12:15 is when things started to go very badly wrong. Pressure in tank 610 was rising through 30 psig and off the scale, which pegged at 55; when control room operators and supervisors ran to have a look at it, they found the tank moving, rumbling, cracking the concrete over it with its vibration and heat expansion, and so hot as to flash cooling water off into steam. One report states that the tank stood on end and fell back again, but did not burst. They ran like hell back to the control room and turned on the VGS system, but couldn't verify that it was working.
It was now 12:30, and clouds of lethal gas were spewing from the plant stack and spreading rapidly through Bhopal. Accounts differ on when the siren was sounded, anywhere from 12:15 to 1 AM, but it was shut off shortly thereafter. Attempts were made to knock down the gas release by spraying water at it, but the sprays couldn't reach high enough to make a difference. One worker was killed when he tried to climb the stack assembly and somehow shut off the release; he was almost immediately overcome by the gas and fell off, breaking several bones. By 1:30, workers were running for their lives: people who lived close to the plant were already dying.
Tank 610 continued to pour MIC and a host of other toxins into the night air until it was empty; some reports mention that the safety valve reclosed (as the pressure fell below 40 psig) around 2:30, and the emission stopped. By now 42 tonnes of deadly gas were flowing through Bhopal, blinding and choking people in their beds.
MIC is heavier than air; it hugs the ground, rolling downhill. The weather conditions on the night of the accident were as bad as they could be: a temperature inversion trapped the gases close to the ground, and there wasn't enough wind to blow the cloud away. There's been considerable controversy over the role played by hydrogen cyanide (HCN) in the deaths at Bhopal: MIC breaks down into HCN at high temperatures, and tank 610 may have reached sufficient temperatures to allow this reaction. Cyanide was found in the bodies of some Bhopal victims, and scientists have merrily argued about which of the many gases making up the lethal cloud was responsible for the deaths, which strikes me as missing the point.
The people of Bhopal were awakened by acute pain in their eyes, noses, and throats; coughing uncontrollably, blinded by tears, vomiting, they fled into the streets to escape. People were trampled to death in the rush to evacuate. Mothers lost their babies when they were literally pulled from their arms by the force of people struggling to push through the crowd. Because MIC is so heavy, concentrations of it were worst right over the ground; the shortest people--children--got the heaviest doses. Many of those who did not die at once succumbed at the grossly unprepared hospitals, drowning as pulmonary edema filled their lungs with fluid or suffocating as their devastated bronchi went into intractable spasm. Doctors had no idea what was responsible for the injuries; eye drops and cough medicine were handed out and glucose drips set up. Bodies were everywhere, piled on one another, littering the streets.
Dawn brought with it evidence of the extent of the disaster. Thousands of bodies--of livestock as well as people--lay where they had fallen. Within a few days every tree in Bhopal lost its leaves, and the grass turned yellow: a blight of biblical proportions. Police trucks carried bodies to be dumped in the river; others were stacked into funeral pyres. Official procedure for identifying the dead was left behind in the rush to clear the city of the dead; we don't know how many people died that night, but initial reports listed the death toll at over two thousand. That figure jumped to 8,000 and then to 10,000 as more and more died of their injuries. All in all, UCIL killed more than twenty thousand people with one accident.
In the wake of the disaster, UCC was faced not only with attempting to address the devastating leak that had occurred, but with preventing another leak. Tonnes of MIC still remained in the other holding tanks, and it was determined that the thing to do was to convert this into Sevin as soon as possible. "Operation Faith" was conducted on December 16, but this time rigorous safety measures were in place and the inhabitants--remaining inhabitants--of Bhopal were evacuated prior to the procedure. Bhopal residents had absolutely no trust left for the authorities; everyone who could fled the city with all their belongings.
It is beyond the scope of this write-up to cover the reaction to Bhopal, or the years which followed. Suffice it to say that this must not be forgotten, that the rest of the world must know about it, tell the next generation what happened. Those who died at Bhopal mattered, and the grossly negligent maintenance and staffing of the UCIL plant that killed them also matters. Remembering Bhopal is remembering that accidents like this can happen, and that the corporations responsible for accidents must make preventing such accidents their priority; that profit does not trump human lives, and that decisions made in a boardroom affect the everyday existence of hundreds of thousands on the other side of the world.
And that's what went wrong.
Information in this post was taken from the following sources:
Eckerman, Ingrid (2004). The Bhopal Saga — Causes and Consequences of the World's Largest Industrial Disaster. India: Universities Press. ISBN 81-7371-515-7. Available via Google Books.
Kalelkar AS, Little AD. (1998) Investigation of Large-magnitude incidents: Bhopal as a Case Study..PDF available. London: The Institution of Chemical Engineers Conference on Preventing Major Chemical Accidents (Arthur D. Little Report)
Labunska I, Stephenson A, Brigden K, Stringer R, Santillo D, Johnston P.A. (1999). The Bhopal Legacy. Toxic contaminants at the former Union Carbide factory site,Bhopal, India: 15 years after the Bhopal accident. PDF available. Greenpeace Research Laboratories, Department of Biological Sciences, University of Exeter, Exeter UK
Stringer R, Labunska I, Brigden K, Santillo D. (2002). "Chemical Stockpiles at Union Carbide India Limited in Bhopal: An investigation". Greenpeace Research Laboratories. PDF available.
Wednesday, June 3, 2009
What warning label where? ValuJet Flight 592
Unless you spend a great deal of time in a chemistry lab or dabble in rocket propulsion, the concept of oxygen as a dangerous substance may not be immediately self-evident. Nor does the word “oxidizer” carry the same weight as, say, “explosive.”
Pressurized pure oxygen was responsible for the vicious rapidity of the flame propagation in the Apollo 1 launchpad fire. More recently, oxygen and the chemical reaction responsible for producing it killed a hundred and ten people and dug a crater in the bedrock of the Florida Everglades.
I was sixteen when ValuJet Flight 592 slammed into the swamp at over five hundred miles an hour. I remember hearing about it, and watching the pictures of the recovery effort on the news. They didn’t find many big pieces of anything, including people; a small amount of human tissue was strongly suspected of belonging to the first officer, but it wasn’t in any condition to provide proof. Eventually 68 of the 110 people aboard were identified. They’re still there, the victims of Flight 592. They’re in the mud, in the cracks in the bedrock, in the murky water.
ValuJet was one of the first low-cost airlines offering cheap fares with no frills, and its fleet was made up of aging McDonnell-Douglas DC-9 and MD-80 jets. It had a contract with several maintenance and repair facilities around the country to perform service and overhauls on its planes, three of which were qualified to provide heavy maintenance. One of these, located in Miami, was SabreTech.
The accident itself
On the afternoon of May 11, 1996, a Douglas DC-9-32, N904VJ, owned and operated by ValuJet Airlines, Inc. as flight 592, took off from Miami International Airport on a flight to William B. Hartsfield Atlanta International. Six minutes later, the crew requested an immediate return to Miami due to smoke in the cockpit and cabin. The interphone connecting the cabin and cockpit wasn’t working (one of many equipment failures plaguing ValuJet planes); contrary to regulations, the flight attendants had to open the door to communicate with the pilots, introducing smoke to the cockpit. Shouts in the background of “fire, fire, fire, fire” can be heard on the recording, coming from the cabin. Just before 2:14 PM, ten minutes after takeoff, the plane vanished from Miami radar.
When emergency personnel arrived at the scene they faced considerable challenges: the wreck site was a quarter-mile from the nearest road, located in a seven-foot-deep swamp in which visibility was approximately nil, and the plane had hit the ground with such force as to render it into lots of tiny little bits, surrounded by mud, sawgrass, and alligators. Nevertheless, through a very great deal of hard work on the part of a large number of searchers and the cooperation of various law enforcement agencies, enough fragments of wreckage were found, identified, and reassembled into a model of the accident aircraft to begin to offer some answers into the cause of the wreck.
Investigators knew that a fire had played some part in the disaster, although where it was located or what had caused it was still unknown. As they pieced together the shreds of the DC-9 fire damage began to appear, located in what had been the forward cargo bay of the plane. Wiring controlling the aircraft’s flight surfaces and engine thrust was burnt through, indicating that the crew had most likely lost control of the plane as the systems died. When the CVR and FDR were finally recovered, the data indicated that progressive control system failure following an initial anomaly had occurred, and this was corroborated by the discovery that the left-side floorboards had melted and collapsed, affecting the captain’s control cables.
Checking with SabreTech and ValuJet records, they found that the forward cargo bay on the accident flight had contained five boxes of "company materials" (COMAT) and a couple of landing-gear wheels, none of which theoretically should have started a fire; however, further investigation revealed that the contents of the COMAT boxes were listed as "Oxy Cannisters [sic] 'Empty'," at which point they began to realize that in all likelihood this had been a completely preventable tragedy.
Emergency oxygen on board commercial passenger airliners is provided not by pressurized oxygen tanks but by chemical oxygen generators. These are cylinders about the size of a tennis-ball can, containing a mixture of sodium chlorate, barium peroxide, and potassium perchlorate. If the cabin loses pressure the compartments holding these things will open, dropping those dinky plastic oxygen masks over the passengers’ heads; pulling on the masks tugs on a lanyard attached to the oxygen generator’s firing pin, setting off a little percussion cap. This produces enough energy to trigger the chemical reaction within the generator core whereby the sodium chlorate is reduced to sodium chloride and oxygen is given off in gas form; it’s a nice, elegant little reaction which does away with the need to carry dangerous pressurized tanks over passengers’ heads and allows the oxygen system to take up very little space.
However, this reaction is exothermic. Powerfully so. An activated oxygen generator is capable of reaching temperatures of five hundred degrees while it’s working; for this reason it is vitally important that when you are carrying these things around or storing them you put a safety cap over the firing pin, preventing them from being triggered by mistake. This would seem to be common sense.
The investigation into ValuJet’s and SabreTech’s shipping and labeling policies and history revealed that not only were the oxygen generators being carried in the accident aircraft’s forward cargo bay not empty or secured for transportation, they were also not appropriately marked, had not been identified as hazardous materials, and were in fact not recognized by maintenance personnel as dangerous. They had been stacked in the cardboard boxes without safety caps, covered with a layer of bubble wrap, and shoved into the cargo bay along with the spare wheels. Apparently these generators had been removed from ValuJet planes when they passed their expiration dates, then left sitting around minus safety caps for several weeks until personnel were told to clean up the storage rooms for an upcoming site visit/audit, whereupon they were packed into boxes–still sans safety caps, as apparently these were unavailable–and sat around some more until someone finally asked if he should send them to Atlanta and was told “okay, that sounds good to me.”
According to the stock clerk, he identified the generators as “empty canisters” because none of the mechanics had talked with him about what they were or what state they were in, and that he had just found the boxes sitting on the floor of the hold area one morning. He said he did not know what the items were. Nobody had bothered to read the ‘reason for removal’ tags on the generators.
Tests on similar oxygen generators in a mockup of the DC-9’s forward cargo bay demonstrated that not only was an activated generator in a cardboard box capable of starting a fire, within ten minutes of ignition the temperature on the ceiling of the cargo bay was reaching temperatures over 3,000 degrees F. Aluminum’s melting point is around 1,220 F, higher or lower depending on the alloy. There was no way the floor of the passenger compartment could withstand this kind of fire.
The forward cargo bay was supposedly fire-resistant due to its lack of ventilation, which would cause a standard fire to use up the available oxygen and burn out fairly quickly. However, not only did the oxygen generators reach ignition temperature, they also, well, generated oxygen, which fed the fire. Regulations didn’t require smoke/fire detection systems in cargo compartments of this type, nor any kind of fire suppression systems.
Going back to the battered black boxes, investigators found that at 2:10 pm, six minutes after takeoff and right before all the electrical systems went to hell, an unidentified sound was recorded on the CVR. According to the FDR, just before the sound, the airplane was climbing through 10,634 feet at 260 knots indicated airspeed. Simultaneous with the noise on the CVR, the FDR recorded a 33-knot decrease in indicated airspeed and a pressure altitude drop of 817 feet. The FDR airspeed and altitude data returned to normal values within 4 seconds. Altitude and speed data recorded on the FDR are based on readings from the static port on the left-hand side of the DC-9 (a small port open to the atmosphere, which registers the pressure of the outside air on the plane as it moves).
An increase of 69 pounds per square foot (psf) sensed by a static pressure sensor on the airplane would result in an 817-foot decrease in altitude (as recorded by the FDR). Further, an increase of 69 psf in static pressure would result in a decrease in airspeed of about 40 knots, which is consistent with a curve fit of the airspeed decrease recorded on the FDR. The brief anomaly in the readings is, therefore, consistent with a momentary jump in the static system pressure. What would cause this sudden pressure increase?
How about a bursting landing-gear tire in the forward cargo bay?
Tests showed that in fact one of the tires recovered from the crash site which was torn open could have produced this level of pressure increase as it blew during the fire. By calculating the length of time it took for the fire to heat up the tire to bursting point in a recreation of the cargo bay, investigators could work out roughly when the fire began–possibly as late as during the airplane’s takeoff roll. Almost immediately after the tire blew, the wiring bundles running under the cabin floor burned through and the crew began to lose control of the plane, as the fire ate its way into the passenger compartment.
Imagine it. You’re in a plane that was built the year Neil Armstrong walked on the moon, bound for Atlanta on a sunny afternoon in May. You’ve been delayed in departure for over an hour and you are probably overjoyed when the damn thing takes off; as usual, you’re looking out the window at the runway flashing by and wondering if the plane is going to make it into the air at all–and, as usual, it does, and the vast hand of inertia presses your butt into your seat as the captain climbs through two thousand feet and begins to bank left. If you’re on the left side of the cabin you can look down and see Miami lazily baking in the afternoon sun.
Then you smell something funny. Something burning. It’s coming from the front of the cabin, and it’s getting worse. People are starting to sound panicky up there, and now there’s flames, visible flames dancing on the floor, and you are in an airplane that is on fire. Perhaps the floor’s gone soft and is beginning to sag, too hot to touch; the carpet’s melting. Flames lick at the seats, and people have begun to scream; and now there’s smoke, black smoke rolling along the ceiling. You can’t get out: there’s nowhere to go. The flight attendants try to alert the cockpit, but the interphone isn’t working. They bang on the door and finally open it–which you absolutely must not do in a case of smoke in the cabin. The oxygen masks have not dropped. By now the crew are losing control and have radioed for an emergency return to Miami, and people are burning alive as the fire spreads and the temperature in the cabin soars. Without control over the engines, flaps, slats, ailerons, or rudder, Flight 592 is helplessly plummeting toward the ground.
Probably the passengers and crew were unconscious by the time of impact, overcome by heat and toxic fumes. Probably none of them were able to see the ground rushing up at them, or feel themselves blown apart by the force of the crash. Had any number of people done their jobs right, it wouldn’t have happened at all; had the SabreTech mechanics properly labeled the generators when they removed them from the aircraft, had they activated them and safely expended the cores as the manufacturer’s and other airlines’ procedures required before shipping them as hazardous materials, this would not have happened. ValuJet and SabreTech had received several warnings as a result of negligent or insufficient safety oversight, and despite the obvious necessity had not made changes to their operating procedures that would have prevented the accident from occurring.
ValuJet never recovered from the crash. In 1997 it merged with low-cost carrier AirTran Airways, and discarded the ValuJet name entirely. Today AirTran’s fleet is among the youngest in the field, with an average age of less than 4 years; in July 09 it will be serving 62 locations in the States. Since ValuJet bought AirTran and took on the AirTran name, the airline has not experienced any fatal accidents and is generally considered among the safest commercial airlines in the country. Lessons learned from the crash wrote new rules regarding oxygen generator disposal, COMAT and hazardous material transportation, compliance inspections, fire detection and suppression systems, and cargo bay design. Flight 592 could have been prevented; the changes made in the industry as a result of the tragedy will hopefully prevent anything like it from happening again.
Information in this post is taken from the official NTSB report.
Pressurized pure oxygen was responsible for the vicious rapidity of the flame propagation in the Apollo 1 launchpad fire. More recently, oxygen and the chemical reaction responsible for producing it killed a hundred and ten people and dug a crater in the bedrock of the Florida Everglades.
I was sixteen when ValuJet Flight 592 slammed into the swamp at over five hundred miles an hour. I remember hearing about it, and watching the pictures of the recovery effort on the news. They didn’t find many big pieces of anything, including people; a small amount of human tissue was strongly suspected of belonging to the first officer, but it wasn’t in any condition to provide proof. Eventually 68 of the 110 people aboard were identified. They’re still there, the victims of Flight 592. They’re in the mud, in the cracks in the bedrock, in the murky water.
ValuJet was one of the first low-cost airlines offering cheap fares with no frills, and its fleet was made up of aging McDonnell-Douglas DC-9 and MD-80 jets. It had a contract with several maintenance and repair facilities around the country to perform service and overhauls on its planes, three of which were qualified to provide heavy maintenance. One of these, located in Miami, was SabreTech.
The accident itself
On the afternoon of May 11, 1996, a Douglas DC-9-32, N904VJ, owned and operated by ValuJet Airlines, Inc. as flight 592, took off from Miami International Airport on a flight to William B. Hartsfield Atlanta International. Six minutes later, the crew requested an immediate return to Miami due to smoke in the cockpit and cabin. The interphone connecting the cabin and cockpit wasn’t working (one of many equipment failures plaguing ValuJet planes); contrary to regulations, the flight attendants had to open the door to communicate with the pilots, introducing smoke to the cockpit. Shouts in the background of “fire, fire, fire, fire” can be heard on the recording, coming from the cabin. Just before 2:14 PM, ten minutes after takeoff, the plane vanished from Miami radar.
When emergency personnel arrived at the scene they faced considerable challenges: the wreck site was a quarter-mile from the nearest road, located in a seven-foot-deep swamp in which visibility was approximately nil, and the plane had hit the ground with such force as to render it into lots of tiny little bits, surrounded by mud, sawgrass, and alligators. Nevertheless, through a very great deal of hard work on the part of a large number of searchers and the cooperation of various law enforcement agencies, enough fragments of wreckage were found, identified, and reassembled into a model of the accident aircraft to begin to offer some answers into the cause of the wreck.
Investigators knew that a fire had played some part in the disaster, although where it was located or what had caused it was still unknown. As they pieced together the shreds of the DC-9 fire damage began to appear, located in what had been the forward cargo bay of the plane. Wiring controlling the aircraft’s flight surfaces and engine thrust was burnt through, indicating that the crew had most likely lost control of the plane as the systems died. When the CVR and FDR were finally recovered, the data indicated that progressive control system failure following an initial anomaly had occurred, and this was corroborated by the discovery that the left-side floorboards had melted and collapsed, affecting the captain’s control cables.
Checking with SabreTech and ValuJet records, they found that the forward cargo bay on the accident flight had contained five boxes of "company materials" (COMAT) and a couple of landing-gear wheels, none of which theoretically should have started a fire; however, further investigation revealed that the contents of the COMAT boxes were listed as "Oxy Cannisters [sic] 'Empty'," at which point they began to realize that in all likelihood this had been a completely preventable tragedy.
Emergency oxygen on board commercial passenger airliners is provided not by pressurized oxygen tanks but by chemical oxygen generators. These are cylinders about the size of a tennis-ball can, containing a mixture of sodium chlorate, barium peroxide, and potassium perchlorate. If the cabin loses pressure the compartments holding these things will open, dropping those dinky plastic oxygen masks over the passengers’ heads; pulling on the masks tugs on a lanyard attached to the oxygen generator’s firing pin, setting off a little percussion cap. This produces enough energy to trigger the chemical reaction within the generator core whereby the sodium chlorate is reduced to sodium chloride and oxygen is given off in gas form; it’s a nice, elegant little reaction which does away with the need to carry dangerous pressurized tanks over passengers’ heads and allows the oxygen system to take up very little space.
However, this reaction is exothermic. Powerfully so. An activated oxygen generator is capable of reaching temperatures of five hundred degrees while it’s working; for this reason it is vitally important that when you are carrying these things around or storing them you put a safety cap over the firing pin, preventing them from being triggered by mistake. This would seem to be common sense.
The investigation into ValuJet’s and SabreTech’s shipping and labeling policies and history revealed that not only were the oxygen generators being carried in the accident aircraft’s forward cargo bay not empty or secured for transportation, they were also not appropriately marked, had not been identified as hazardous materials, and were in fact not recognized by maintenance personnel as dangerous. They had been stacked in the cardboard boxes without safety caps, covered with a layer of bubble wrap, and shoved into the cargo bay along with the spare wheels. Apparently these generators had been removed from ValuJet planes when they passed their expiration dates, then left sitting around minus safety caps for several weeks until personnel were told to clean up the storage rooms for an upcoming site visit/audit, whereupon they were packed into boxes–still sans safety caps, as apparently these were unavailable–and sat around some more until someone finally asked if he should send them to Atlanta and was told “okay, that sounds good to me.”
According to the stock clerk, he identified the generators as “empty canisters” because none of the mechanics had talked with him about what they were or what state they were in, and that he had just found the boxes sitting on the floor of the hold area one morning. He said he did not know what the items were. Nobody had bothered to read the ‘reason for removal’ tags on the generators.
Tests on similar oxygen generators in a mockup of the DC-9’s forward cargo bay demonstrated that not only was an activated generator in a cardboard box capable of starting a fire, within ten minutes of ignition the temperature on the ceiling of the cargo bay was reaching temperatures over 3,000 degrees F. Aluminum’s melting point is around 1,220 F, higher or lower depending on the alloy. There was no way the floor of the passenger compartment could withstand this kind of fire.
The forward cargo bay was supposedly fire-resistant due to its lack of ventilation, which would cause a standard fire to use up the available oxygen and burn out fairly quickly. However, not only did the oxygen generators reach ignition temperature, they also, well, generated oxygen, which fed the fire. Regulations didn’t require smoke/fire detection systems in cargo compartments of this type, nor any kind of fire suppression systems.
Going back to the battered black boxes, investigators found that at 2:10 pm, six minutes after takeoff and right before all the electrical systems went to hell, an unidentified sound was recorded on the CVR. According to the FDR, just before the sound, the airplane was climbing through 10,634 feet at 260 knots indicated airspeed. Simultaneous with the noise on the CVR, the FDR recorded a 33-knot decrease in indicated airspeed and a pressure altitude drop of 817 feet. The FDR airspeed and altitude data returned to normal values within 4 seconds. Altitude and speed data recorded on the FDR are based on readings from the static port on the left-hand side of the DC-9 (a small port open to the atmosphere, which registers the pressure of the outside air on the plane as it moves).
An increase of 69 pounds per square foot (psf) sensed by a static pressure sensor on the airplane would result in an 817-foot decrease in altitude (as recorded by the FDR). Further, an increase of 69 psf in static pressure would result in a decrease in airspeed of about 40 knots, which is consistent with a curve fit of the airspeed decrease recorded on the FDR. The brief anomaly in the readings is, therefore, consistent with a momentary jump in the static system pressure. What would cause this sudden pressure increase?
How about a bursting landing-gear tire in the forward cargo bay?
Tests showed that in fact one of the tires recovered from the crash site which was torn open could have produced this level of pressure increase as it blew during the fire. By calculating the length of time it took for the fire to heat up the tire to bursting point in a recreation of the cargo bay, investigators could work out roughly when the fire began–possibly as late as during the airplane’s takeoff roll. Almost immediately after the tire blew, the wiring bundles running under the cabin floor burned through and the crew began to lose control of the plane, as the fire ate its way into the passenger compartment.
Imagine it. You’re in a plane that was built the year Neil Armstrong walked on the moon, bound for Atlanta on a sunny afternoon in May. You’ve been delayed in departure for over an hour and you are probably overjoyed when the damn thing takes off; as usual, you’re looking out the window at the runway flashing by and wondering if the plane is going to make it into the air at all–and, as usual, it does, and the vast hand of inertia presses your butt into your seat as the captain climbs through two thousand feet and begins to bank left. If you’re on the left side of the cabin you can look down and see Miami lazily baking in the afternoon sun.
Then you smell something funny. Something burning. It’s coming from the front of the cabin, and it’s getting worse. People are starting to sound panicky up there, and now there’s flames, visible flames dancing on the floor, and you are in an airplane that is on fire. Perhaps the floor’s gone soft and is beginning to sag, too hot to touch; the carpet’s melting. Flames lick at the seats, and people have begun to scream; and now there’s smoke, black smoke rolling along the ceiling. You can’t get out: there’s nowhere to go. The flight attendants try to alert the cockpit, but the interphone isn’t working. They bang on the door and finally open it–which you absolutely must not do in a case of smoke in the cabin. The oxygen masks have not dropped. By now the crew are losing control and have radioed for an emergency return to Miami, and people are burning alive as the fire spreads and the temperature in the cabin soars. Without control over the engines, flaps, slats, ailerons, or rudder, Flight 592 is helplessly plummeting toward the ground.
Probably the passengers and crew were unconscious by the time of impact, overcome by heat and toxic fumes. Probably none of them were able to see the ground rushing up at them, or feel themselves blown apart by the force of the crash. Had any number of people done their jobs right, it wouldn’t have happened at all; had the SabreTech mechanics properly labeled the generators when they removed them from the aircraft, had they activated them and safely expended the cores as the manufacturer’s and other airlines’ procedures required before shipping them as hazardous materials, this would not have happened. ValuJet and SabreTech had received several warnings as a result of negligent or insufficient safety oversight, and despite the obvious necessity had not made changes to their operating procedures that would have prevented the accident from occurring.
ValuJet never recovered from the crash. In 1997 it merged with low-cost carrier AirTran Airways, and discarded the ValuJet name entirely. Today AirTran’s fleet is among the youngest in the field, with an average age of less than 4 years; in July 09 it will be serving 62 locations in the States. Since ValuJet bought AirTran and took on the AirTran name, the airline has not experienced any fatal accidents and is generally considered among the safest commercial airlines in the country. Lessons learned from the crash wrote new rules regarding oxygen generator disposal, COMAT and hazardous material transportation, compliance inspections, fire detection and suppression systems, and cargo bay design. Flight 592 could have been prevented; the changes made in the industry as a result of the tragedy will hopefully prevent anything like it from happening again.
Information in this post is taken from the official NTSB report.
Subscribe to:
Comments (Atom)